INTRODUCTION
The nose is centrally located on the face and significantly contributes to an individual’s overall appearance. Consequently, any surgical intervention involving the nose must prioritise the achievement of optimal results, which encompass skin colour matching, adequate tissue coverage, flap viability, and aesthetically acceptable outcomes.1 A modification of the Rintala glabellar linear advancement flap was used in the treatment of basal cell carcinoma located in the nasal region.2
CASE PRESENTATION
An 87-year-old female patient was referred to the authors’ department, having a diagnosis of basal cell carcinoma situated in the middle one-third of the nasal dorsum (Figure 1A). The tumour was excised using a modified Rintala flap technique. The flap design, elevation, and transfer were carried out in accordance with the traditional Rintala flap procedure while utilising local anaesthesia. The resultant defect measured 1×1 cm (Figure 1B).3,4 A superior rectangular flap was designed, extending to the central forehead. The flap was elevated in the supraperiosteal plane, with bilateral parallel incisions made along both sides of the nasal sidewall, from the corners of the defect to the glabellar region and into the forehead, thereby enhancing the advancement of the flap (Figure 1C–E). Burow’s triangle resection was deemed unnecessary due to the considerable elasticity of the skin, and the suturing
was executed without applying increased tension.
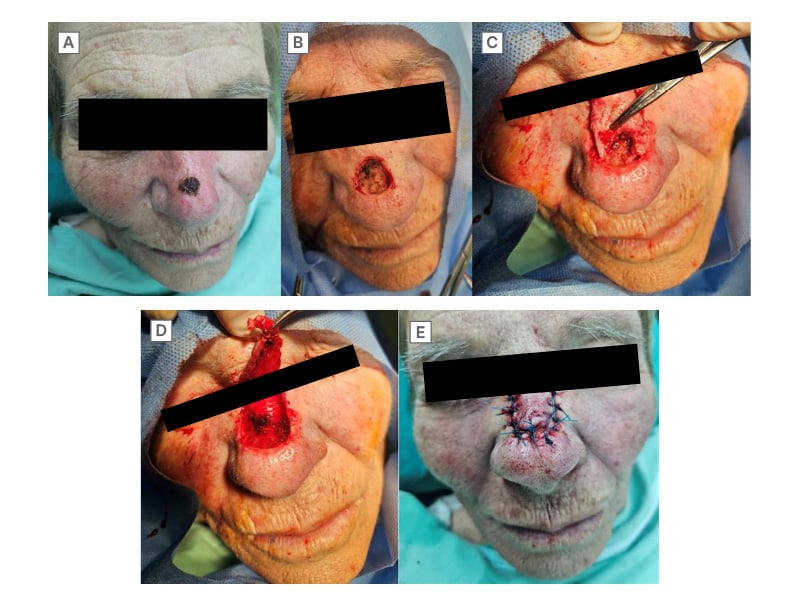
Figure 1: Patient with basal cell carcinoma and modified Rintala flap.
The post-operative wound healing procedure was completed without any complications such as infections, hypertrophic scars, keloids, or delayed closure of the trauma. In addition to a rapid recovery, a highly satisfactory aesthetic result was observed during the follow-up visits at 15 and 30 days after surgery.
CONCLUSION
The Rintala flap, initially described in 1969, serves as a dependable option for the reconstruction of moderate nasal defects by utilising an advancement flap from the central forehead.3 A significant limitation of this technique is the potential for ischaemia at the distal end of the flap.5 Consequently, the acceptable range for flap transfer is defined from the glabella to the middle third of the nasal dorsum. It is crucial to recognise that the resection of Burow’s triangles, whether performed below the eyebrow or in the canthal region, may result in deformities, thereby restricting the distance that the flap can be advanced. Through the implementation of the modified Rintala technique, as previously outlined, it is possible to successfully enhance the width of the rectangle along the nasal dorsum while avoiding the creation of Burow’s triangles. This method provides aesthetically favourable outcomes without introducing distortions to the central facial region.





