Meeting Summary
According to USA data, around 15% of patients with endometrial cancer (EC) have advanced disease at diagnosis, which is associated with poor survival rates and a high risk of recurrence. This symposium explored treatment strategies in advanced EC (aEC), focusing on the key role of immunotherapy in combination with targeted treatment such as the tyrosine kinase inhibitor (TKI), levatinib. Experts provided important real-world insights into treatment decision-making and the management of adverse events in order to optimise outcomes for patients.
Treatment Approaches in Advanced Endometrial Cancer: The Impact of Immunotherapy Plus Targeted Treatment
Endometrial Cancer: Where Do We Stand?
Christian Marth, Head of the Department of Obstetrics and Gynaecology at Innsbruck Medical University in Austria, explained that EC incidence has risen steadily over recent years, particularly in countries with a high sociodemographic index.1 At the time of diagnosis in the USA, approximately 15% of patients have advanced disease,2 which is associated with 5-year survival rates of only 20–60%3,4 and a high risk of recurrence.5,6 Until recently, standard first-line treatment for advanced or recurrent EC was platinum-based chemotherapy (± radiotherapy).7 However, as Marth highlighted, there remains a lack of consensus on the optimal second-line treatment approach for patients with EC who have previously received platinum-containing chemotherapy.7-10
Lenvatinib + Pembrolizumab: Outcomes in Endometrial Cancer
Improved outcomes achievable with immune checkpoint inhibitors (ICI) added to chemotherapy have shifted this treatment landscape, positioning combination therapy as the new preferred first-line option for mismatch repair deficient (dMMR) tumours.8 In clinical trials, ICIs achieved overall response rates (ORR) of 40–50% in dMMR patients, but responses remained relatively low in the non-dMMR population (approximately 15%).11,12 In an attempt to boost efficacy in non-dMMR patients, pembrolizumab has been evaluated in combination with the TKI lenvatinib.13,14 As Marth explained, there is a good rationale for combining these two agents, as lenvatinib not only blocks tumour angiogenesis but has additional actions, such as increasing CD8+ T cell function and inhibiting T cell exhaustion, that augment ICI activity.15-17
Lenvatinib + pembrolizumab was directly compared to chemotherapy (doxorubicin or paclitaxel) in the KEYNOTE-775 multicentre, open-label, randomised, Phase III trial in patients with advanced, metastatic, or recurrent EC who have previously received ≥1 platinum-based chemotherapy.14 Results showed a significant survival benefit for the ICI/TKI combination versus chemotherpay in non-dMMR patients and all comers.
Progression-free survival (PFS) in non-dMMR patients was improved from 3.8 months with chemotherapy to 6.7 months with lenvatinib + pembrolizumab (hazard ratio [HR]: 0.60; 95% CI: 0.50–0.72), while overall survival (OS) was increased from 12.2 months with chemotherapy to 18.0 months with lenvatinib + pembrolizumab (HR: 0.70; 95% CI: 0.58–0.83), respectively.18 Both ORR and complete response (CR) in non-dMMR patients were more than doubled in the lenvatinib + pembrolizumab arm versus chemotherapy, and duration of response was also extended.18 The ORR was 32.4% versus 15.1%, respectively, with CR rates of 5.8% versus 2.6%.
As Marth explained, efficacy in the overall patient population of KEYNOTE-775 was enhanced because of the higher responsiveness of dMMR patients. HRs for PFS and OS for lenvatinib + pembrolizumab versus chemotherapy in the overall patient population were 0.56 (95% CI: 0.48–0.66) and 0.65 (95% CI: 0.55–0.77), respectively, with an increase in CR rates from 2.6% to 7.5% and prolongation of duration of response compared with chemotherapy.18 Sub-group analysis of OS in KEYNOTE-775 by histology showed a benefit of lenvatinib + pembrolizumab over chemotherapy across endometrioid, serous, and clear cell subtypes of EC, although this was not powered to show statistical significance.19 Median PFS on the next line of therapy (PFS2) for lenvatinib + pembrolizumab was significantly greater than that of physician’s choice treatment, 14.4 months versus 9.8 months, respectively (p<0.0001).20 Overall safety results from the KEYNOTE-775 trial showed a greater number of dose reductions (67% versus 13%) and dose discontinuations (39% versus 8%) due to adverse events (AE) with lenvatinib + pembrolizumab versus chemotherapy.18
Immune Checkpoint Inhibitors in Combination with Chemotherapy
In what Marth described as “a major effort to bring ICIs into the first-line setting,” several studies have evaluated first-line combination therapy with platinum-based chemotherapy in aEC. The RUBY-1,21 NRG-GY018,22 and DUO-E23 studies demonstrated that the addition of ICI to first-line chemotherapy prolonged PFS with a notable benefit in dMMR tumours, with HRs versus chemotherapy alone ranging between 0.28 (95% CI: 0.16–0.50) and 0.42 (95% CI: 0.22–0.80). Marth additionally highlighted the flattening of the tail of the Kaplan-Meier survival curves with ICI plus chemotherapy in these studies. The PFS signal was also positive in the non-dMMR population, although not as pronounced as the efficacy results in dMMR patients, with HRs between 0.54 (95% CI: 0.41–0.71) and 0.77 (95% CI: 0.60–0.97) for single-agent ICI plus chemotherapy. Currently, there are no statistically significant OS data from these studies in non-dMMR patients; however, among the ICIs, RUBY-1 is the only trial to have met its dual primary OS endpoint in the intention-to-treat population (HR: 0.69; 95% CI: 0.54–0.89).24-27
Although chemotherapy is undoubtedly effective in dMMR tumours, Marth queried whether it is really needed when treating with ICIs.28 Real-world evidence indicates that 58% of oncologists rechallenge with platinum-based chemotherapy in the second-line setting,29 but this treatment approach is associated with poor response rates.30 When comparing across clinical trials, chemotherapy also appears to be the main driver of toxicity in combinations with ICIs.25 Although ICIs are associated with some specific immune-related side effects such as hypothyroidism and rash, Marth described these as “typically mild and manageable,” noted Marth.
The ENGOT-en9/LEAP-001 Trial
Against this backdrop, the ENGOT-en9/LEAP-001 trial evaluated first-line lenvatinib + pembrolizumab in patients with advanced or recurrent EC who were chemotherapy-naïve except for one prior line of neoadjuvant platinum-based chemotherapy.31 This trial was negative, with lenvatinib + pembrolizumab failing to meet the primary endpoint of improved PFS versus platinum-based chemotherapy. Hence, no claims can be made from this study. In non-dMMR patients who had received prior (neo)adjuvant chemotherapy lenvatinib+pembrolizumab reported benefit, with median PFS of 12.5 months versus 8.3 months for chemotherapy (HR: 0.60; 95% CI: 0.37–0.97) and median OS of 34.2 versus 21.1 months, respectively (HR: 0.67; 95% CI: 0.41–1.11; Figure 1).31 As with KEYNOTE-775, more dose reductions and discontinuations due to AEs occurred with lenvatinib + pembrolizumab compared with chemotherapy, but as Marth pointed out, this was continuous therapy as opposed to a fixed number of chemotherapy cycles (≤7).31
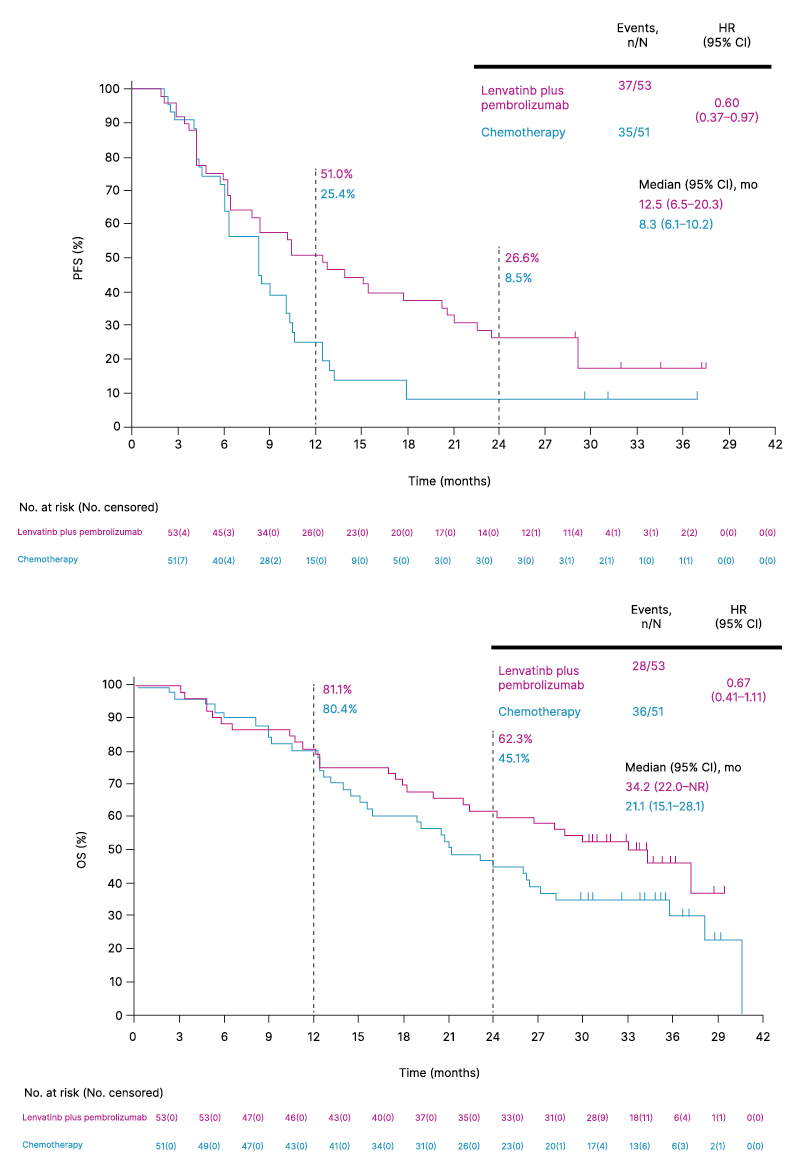
Figure 1: ENGOT-en9/LEAP-001: progression-free survival and overall survival in patients treated with prior (neo)adjuvant chemotherapy.31
HR: hazard ratio; mo: months; NR: not reached; OS: overall survival; PFS: progression-free survival.
Considering the treatment positioning for lenvatinib + pembrolizumab, Marth suggested this combination could be a potential first-line option in the advanced/metastatic setting for any patient who has received prior (neo)adjuvant chemotherapy, due to the high degree of platinum resistance seen in EC tumours. It can also be used in the second-line setting after first-line chemotherapy plus ICI, as per the licensed indication for lenvatinib in patients who have received prior platinum-containing chemotherapy.
Patient Selection: Individualising Treatment Decisions to Optimise Outcomes
Biomarkers Influencing Treatment Selection
Whether an EC tumour is ‘hot’ or ‘cold’ is a key driver of treatment choice. Isabelle Ray-Coquard, Professor at the Léon Bérard Centre in Lyon, France, explained that ICIs are the current backbone of therapy for hot tumours such as DNA polymerase epsilon (POLE)-mutated and dMMR ECs. In contrast, ICIs show limited efficacy in cold tumours, including no specific molecular profile (NSMP) and p53 wild-type/mutated ECs, and therefore, combination therapy is required.32,33
In the current ESGO-ESTRO-ESP guidelines, first-line therapy for patients with advanced or recurrent EC with no prior chemotherapy (except in the adjuvant setting) is directed primarily based on dMMR status.8 For dMMR tumours, chemotherapy plus ICI is recommended. For non-dMMR tumours, treatment choice depends on disease aggressiveness. For the majority of patients with symptomatic advanced disease or rapidly growing recurrent disease, chemotherapy is recommended as first-line. In cases where chemotherapy is contraindicated or patients have recurrent EC after prior platinum-containing chemotherapy in the (neo)adjuvant setting, the combination of pembrolizumab + lenvatinib is recommended. Ray-Coquard also emphasised the importance of local treatment in addition to systemic therapy to help relieve symptoms and improve patient outcomes.8
The Key Role of Molecular Analysis
Molecular analysis is important both at initial diagnosis and in the relapse setting in EC, as biomarkers provide key treatment-relevant insights into underlying disease pathology and genomics. Ray-Coquard explained that initial sequencing of POLE is vital because these pathogenic mutations strongly influence disease prognosis and can mimic p53 mutations or dMMR. Patients who are POLE-negative should undergo MMR immunohistochemistry or microsatellite instability testing to determine dMMR status. For non-dMMR tumours, further immunohistochemistry is required to pinpoint any aberrations/mutations in p53. Applying these principles of molecular analysis, therefore, results in four possible histology subtype-independent EC diagnoses: POLE mutation, dMMR, NSMP, or p53 mutation.34,35 Beyond the biomarkers currently recommended for testing in EC, Ray-Coquard also noted that the patients’ hormone receptor status is likely to become increasingly important moving forward as clinical trials in this area advance.
The molecular classification algorithm described was applied in post-hoc analysis of the RUBY trial of ICI (dostarlimab) plus chemotherapy for advanced or recurrent EC.36 In the 22% of the trial population with p53 mutations, significant improvements in PFS (HR: 0.55; 95% CI: 0.30–0.99) and OS (HR: 0.41; 95% CI: 0.20–0.82) were seen with the addition of ICI to chemotherapy. In contrast, exploratory biomarker subgroup analysis of the DUO-E trial showed no predictive effect of p53 mutations on ICI (durvalumab) efficacy as measured by PFS.37 However, Ray-Coquard noted that, at 59%, the incidence of p53 mutations was substantially higher in this trial than in RUBY, and the non-dMMR population was heterogeneous, with a large overlap of biomarkers.
In terms of the impact of p53 mutation status on the efficacy of other therapeutic agents, Ray-Coquard pointed to sub-analyses of the RUBY Part 2 and DUO-E studies, which indicate that p53 mutations may be predictive of poly(ADP ribose) polymerase inhibitor (PARPi) activity.37,38 In contrast, biomarker analysis of the KEYNOTE-146 study by status of selected genes revealed no difference in ORR for the pembrolizumab-lenvatinib combination in p53-mutated versus unmutated (NSMP/p53 wild-type) patients (Figure 2).39 KEYNOTE-146 was a Phase Ib/II, open-label, single-arm, multicentre study that evaluated response to pembrolizumab-lenvatinib in patients with select solid tumours, including previously treated advanced EC. In a reflection of this evidence, current French guidelines do not incorporate p53 (or any alternative biomarker) as a factor for determining patient eligibility for immunotherapy in the aEC setting.40
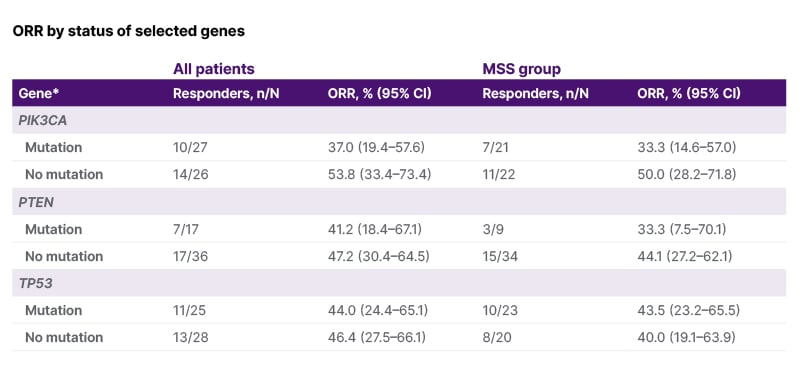
Figure 2: KEYNOTE-146: Biomarker analysis of pembrolizumab-lenvatinib.39
*Hotspot mutations in PIK3CA (oncogene) and deleterious mutations in PTEN or TP53 (tumour suppressor genes).
MSS: microsatellite stable; ORR: objective response rate.
Looking at the broader picture, Ray-Coquard summarised current biomarkers and prognostic factors that can be used to guide therapeutic decision-making in EC (Figure 3). First, it is important that all patients with EC undergo comprehensive molecular profiling, as this provides insights into patient prognosis and optimal treatment pathways. In addition to molecular biomarkers, important non-molecular characteristics that influence treatment choice include prior therapy, patient comorbidities, and toxicity.34,35
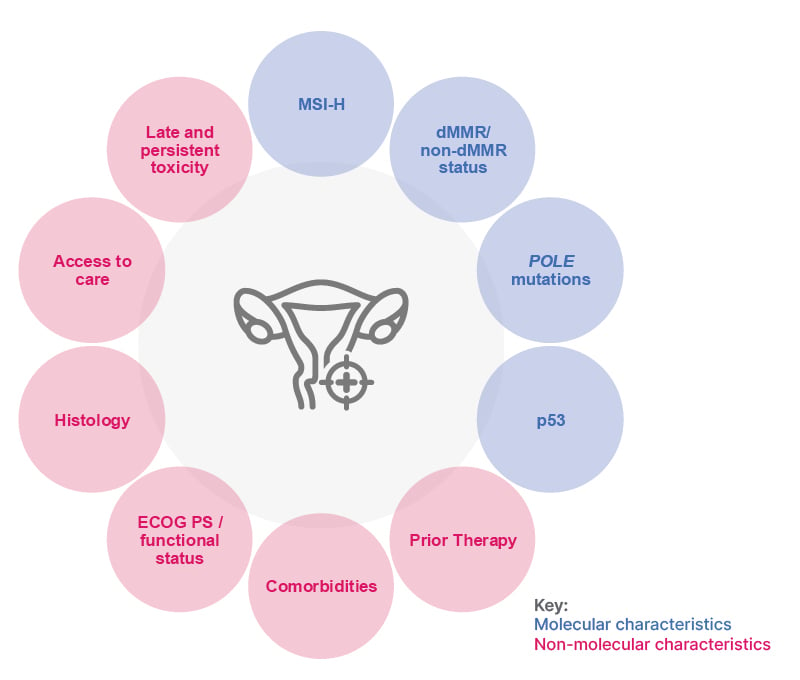
Figure 3: Patient characteristics influencing treatment choice in endometrial cancer.34,35
dMMR: deficient mismatch repair; ECOG PS: Eastern Cooperative Oncology Group performance status; MSI-H: microsatellite instability-high; POLE: DNA polymerase epsilon.
Managing Patients on Immunotherapy plus Targeted Treatment: Real-World Cases
Defining Risk and Selecting Treatment
Vanda Salutari from Fondazione Policlinico Universitario A. Gemelli-IRCCS in Rome, Italy, explained that patients with EC treated in clinical practice constitute a heterogeneous population and are very different to the “perfect” patients enrolled in trials. She went on to present a real patient case study of EC with AEs, adapted for educational purposes. Patient A was a 58-year-old female diagnosed with primary International Federation of Gynaecology and Obstetrics (FIGO) prognostic Stage IIIC G2-G3 EC. Molecular classification was non-dMMR status with mutated p53, making her a high-risk patient according to the updated ESGO-ESTRO-ESP definition of risk groups.8 Patient A underwent treatment with carboplatin–paclitaxel chemotherapy followed by external-beam radiotherapy. Follow-up after 8 months showed symptoms consistent with disease recurrence, while a physical exam and CT scan revealed a pelvic mass with peritoneal carcinomatosis.
ESGO-ESTRO-ESP 2025 guidelines currently recommend lenvatinib + pembrolizumab for first-line systemic therapy in unresectable Stage III/IV or recurrent EC if chemotherapy is contraindicated in patients with non-dMMR relapsed disease and with prior chemotherapy in the adjuvant/neoadjuvant setting.8 This recommendation is based on a subgroup analysis of the LEAP-01 study, which reported PFS benefit for lenvatinib + pembrolizumab in the non-dMMR population and all-comers previously treated with (neo)adjuvant therapy.31 Salutari also questioned what a contraindication to chemotherapy actually means in the context of current guidelines, suggesting it could encompass early and severe disease recurrence as well as toxicity, as seen in the case of patient A. In addition, the platinum-free interval in EC appears to have less clinical impact than in other gynaecological cancers, with limited evidence in the literature to show that a longer platinum-free interval correlates with platinum rechallenge response.41
Optimising Adverse Event Management
For patient A (this is a real patient case anonymised with AEs adapted for educational purposes), the multidisciplinary team decision was to introduce treatment with lenvatinib + pembrolizumab. Within the first few weeks, the patient developed Grade 2 persistent hypertension, which was managed with medication, and Grade 1 fatigue and diarrhoea, which was treated with probiotics, loperamide, and a banana-rice-apple sauce-toast (BRAT) diet. A CT scan showed a partial response. However, after treatment cycle 4, patient A developed decreased appetite (Grade 2), weight loss, and fatigue, which became intolerable. Salutari acknowledged that this type of toxicity can substantially impact the patient’s quality of life (QoL). Although temporary dose adjustment/cessation of lenvatinib can be considered given its role in inducing weight loss, Salutari stressed that it is important to be proactive, recognising when patients are experiencing weight loss and intervening early in order to avoid dose reductions/interruptions wherever possible.42 Weight loss in these cases is typically muscle, not fat, and reduced muscle mass can have negative consequences for oncology patients, given its association with poor QoL, disease progression, treatment toxicity, and shorter survival. For patients like patient A, consideration can therefore be given to supplementing the diet with high-calorie, high-protein nutritional supplements or meal replacement shakes to help meet energy needs. Gastrointestinal symptoms such as nausea, early satiety, and dyspepsia, which may contribute to reduced food intake, should also be addressed. Finally, there is the option to prescribe antiemetic medications such as ondansetron or metoclopramide to alleviate nausea and improve appetite.43 In patient A’s case, the decision was taken to reduce the lenvatinib dose to 14 mg to counter persistent and intolerable Grade 2 weight loss and fatigue. Subsequent CT scans showed the partial response was maintained, and she remained on lenvatinib + pembrolizumab treatment for over a year.
Considering the real dose-limiting toxicity of the lenvatinib + pembrolizumab combination, Salutari noted that because overlapping AEs such as fatigue, appetite loss, and arthralgia can all impact QoL, it is important to educate patients and caregivers to detect these symptoms early. Careful management of AEs with prevention strategies, early detection, and proactive interventions allows patients to remain on the full dose of lenvatinib as long as possible in order to gain maximal benefit from treatment. When managing toxicity with lenvatinib + pembrolizumab and other targeted therapies, Salutari urged oncologists to “make friends” because specialities such as cardiologists, endocrinologists, neurologists, nutritionists, and gastroenterologists can all help in optimising treatment outcomes for patients with EC.
| Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard or by searching for the MHRA Yellow Card in the Google Play or Apple App Store. For Republic of Ireland: www.hpra.ie. Adverse events should also be reported to Eisai Ltd on +44 (0)208 600 1400 or [email protected].. |
Document Number: EMEA-ONC-25-00137
Date of Preparation: September 2025






