Abstract
Mycoplasma pneumoniae (MP) is a well-known respiratory pathogen that can lead to various extrapulmonary complications, including a rare form of MP-induced rash and mucositis. This case report discusses a 24-year-old male who presented with symptoms of oral mucosal swelling, sore throat, cough, and dysphagia following a recent tooth extraction. He received initial empirical therapy with amoxicillin-clavulanate, which failed to alleviate symptoms, necessitating further workup. This case initially raised concerns about other potential causes of oral ulcers (e.g., viral infections, Stevens–Johnson syndrome). However, the diagnosis was established by means of PCR testing for MP on a throat swab specimen, while blood cultures for Group A Streptococcus were negative. The patient subsequently received azithromycin with metronidazole and was advised to use nystatin mouthwash. Remarkably, he experienced complete resolution of mucositis symptoms within 2 weeks, with only mild residual pigmentation noted on follow-up. This case underscores the importance of recognising MP-induced mucositis, which can be easily misdiagnosed as Stevens–Johnson syndrome. It highlights the necessity for precise diagnostic methods and timely intervention to ensure optimal patient outcomes.
Key Points
1. Mycoplasma pneumoniae-induced rash and mucositis (MIRM) is a rare but important differential for severe mucocutaneous eruptions. Accurate differentiation from Stevens–Johnson syndrome is crucial, as MIRM has a distinct infectious trigger and a more favourable prognosis.2. MIRM is characterised by prominent mucosal involvement with limited skin detachment. This case, diagnosed using established clinical criteria and PCR testing, demonstrated rapid improvement with macrolide therapy. PCR testing for M. pneumoniae is essential for diagnosis in patients presenting with severe mucositis, even without radiographic pneumonia.
3. While most patients with MIRM recover fully, mucosal sequelae can occur. The authors’ patient achieved complete mucosal healing within 2 weeks, with only transient hyperpigmentation. MIRM typically follows a benign course with macrolide treatment, but follow-up is recommended to monitor potential ocular or genital complications.
CASE PRESENTATION
A 24-year-old male with no history of immune deficiency, diabetes, or drug allergies presented to the emergency department. He experienced oral swelling and a dry cough. He denied any recent travel. His symptoms began 4 days earlier with a sore throat, dry cough, tooth pain, and whitish mucus in his mouth. The oral swelling, which was mild at first, gradually worsened and caused dysphagia. Notably, he had a tooth extraction a week prior without prophylactic antibiotics. In the emergency department, he was empirically covered with broad-spectrum amoxicillin-clavulanate, along with acetaminophen for symptom relief, pending further diagnostic evaluation. On examination, the patient was alert, oriented, and febrile (38.3 °C), with a heart rate of 92 bpm and a blood pressure of 120/70 mmHg. No significant signs of systemic involvement, such as hypotension or tachycardia, were observed. Oral examination revealed congested mucosa, a whitish membrane over the tonsils, and an oral ulcer with black discolouration, as shown in Figure 1.

Figure 1: Oral mucosal ulcerations on the buccal mucosa and tongue, consistent with Mycoplasma pneumoniae-induced mucositis.
The oral mucosa appeared congested, with erythematous patches, ulcerative lesions, and areas covered by a whitish pseudomembrane (Day 1). The patient presented with erythematous patches and ulcerative lesions that gradually improved following treatment with azithromycin.
INVESTIGATIONS
The white blood cell (WBC) count was mildly elevated (13.7×10⁹ /L), and the C-reactive protein (CRP) level was 79.1 mg/L (reference: <5 mg/L), indicating a significant inflammatory response consistent with infection. Liver and renal function tests were within normal limits. Blood and throat cultures were negative for Group A Streptococcus; however, PCR testing of a throat swab confirmed the presence of Mycoplasma pneumoniae (MP). The chest X-ray was unremarkable, with no evidence of consolidation.
TREATMENT
The patient was admitted to the general medical ward and was started on treatment. Blood and throat cultures were ordered, and amoxicillin-clavulanate was discontinued as the authors decided to wait for the culture results before starting antibiotics. Acetaminophen was administered as needed, and an urgent dermatologist consultation was arranged. Once the PCR test results for MP on a throat swab specimen returned positive, the patient was commenced on intravenous (IV) azithromycin 500 mg daily for 5 days. Additionally, metronidazole 500 mg three times daily was prescribed for 5 days due to the possibility of secondary anaerobic infection following the patient’s recent dental procedure, although no confirmed bacterial superinfection was identified. Nystatin mouthwash was also initiated empirically to cover potential fungal infection.
FOLLOW-UP AND OUTCOMES
The patient demonstrated rapid clinical improvement, with complete resolution of mucositis symptoms within 2 weeks, evidenced by the disappearance of oral ulcers and pseudomembranous ulcers. Mild post-inflammatory hyperpigmentation persisted as the only residual finding. Laboratory markers showed significant improvement: CRP levels normalised from 79.1 mg/L to 8.2 mg/L, while the WBC count decreased from 13.7×10⁹ /L to 11.5×10⁹ /L. During the 4-week follow-up, both inflammatory markers had completely normalised (CRP: <5 mg/L; WBC: 5.2×10⁹ /L), with no evidence of active mucosal lesions.
Follow-up diagnostics revealed normal findings, including the resolution of the previously noted oral mucosal ulcers and a return to baseline appearance of the throat and buccal mucosa. No signs of active infection or new lesions were observed (Figure 2).

Figure 2: Mild oral pigmentation during mucositis healing.
At the 2-week follow-up, mild pigmentation was observed on the buccal mucosa. This residual pigmentation was a normal finding in the healing process of oral mucositis and did not suggest scarring or further complications.
During the 4-week follow-up, mild pigmentation was noted on the buccal mucosa. This was attributed to the healing process and was not associated with scarring. The pigmentation was considered a normal variation following mucosal ulceration and did not require further monitoring (Figure 3).
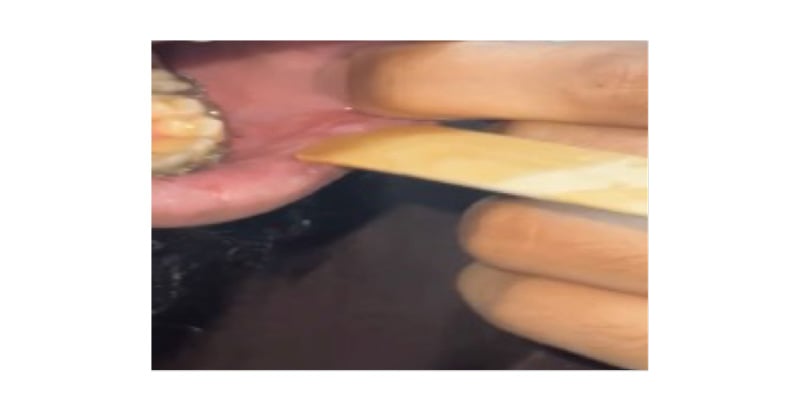
Figure 3: Complete resolution of mucositis buccal mucosa.
DISCUSSION
MP is a well-known respiratory pathogen that can lead to various intrapulmonary and extrapulmonary complications, including a rare mucocutaneous entity termed MP-induced rash and mucositis (MIRM).1,2 Extrapulmonary complications occur in approximately 25% of MP infections, and can affect multiple systems, including dermatological, gastrointestinal, cardiovascular, neurological, haematological, and musculoskeletal systems.3 Among these, dermatological complications are relatively rare, accounting for only 1–5% of cases.4 Common cutaneous manifestations include exanthematous eruptions, erythema nodosum, urticaria, and erythema multiforme major or Stevens–Johnson syndrome (SJS).5,6 Less frequently, bullous erythema multiforme, pityriasis rosea, toxic epidermal necrolysis (TEN), and mucositis are observed.7 Both cutaneous and mucosal involvement have been reported in MIRM, though mucosal manifestations, such as oral ulcers and erythematous patches, are commonly observed. Cutaneous findings like rash and lesions may accompany mucosal involvement but are less frequently observed in the absence of systemic involvement.
The authors’ patient developed oral mucosa swelling concurrently with cough and sore throat. The swelling was progressive and associated with dysphagia. An oral ulcer with a black, reddish spot developed. There was no involvement of the ocular, genital, or skin mucosa. The patient’s presentation raised initial concern for SJS, prompting microbiological testing. The testing, including a respiratory panel multiplex PCR, was positive for MP, confirming the diagnosis of MIRM. The patient started as an inpatient on IV azithromycin 500 mg, nystatin, IV fluid, and acetaminophen. He was discharged with 500 mg of azithromycin for an additional 2 days to complete a 5-day course of antibiotics. He was educated about good oral hygiene, and 2 weeks later was followed as an outpatient. He showed complete recovery of the swelling and ulcers, with only mild pigmentation seen following these lesions. This case exemplifies several classic features of MIRM: predominant mucosal involvement without significant cutaneous lesions, a clear infectious trigger (MP), rapid response to macrolide therapy, and complete resolution.
MIRM was established as a distinct clinical entity from erythema multiforme and SJS/TEN in 2015 by Canavan et al.2 It primarily involves mucosal sites, especially oral (94%), ocular (82%), and genital (63%) mucosa.2,8 Unlike SJS/TEN, MIRM typically presents in younger males and lacks significant skin involvement. Cutaneous findings, if present, are pleomorphic and commonly consist of vesicles or bullous lesions (77%), targetoid lesions (48%), and, less frequently, papular, macular, or morbilliform lesions.9 Accurate differentiation between MIRM and other mucocutaneous disorders, such as SJS/TEN, is vital due to differences in prognosis and management.10 SJS/TEN typically presents in adult females, with large purpuric necrotic lesions triggered by drugs such as allopurinol, lamotrigine, anticonvulsants, sulfonamides, and non-steroidal anti-inflammatory drugs.11 In contrast, MIRM is associated with direct infectious triggers and an immunopathogenesis involving immune complex deposition, complement activation, or molecular mimicry.12
Canavan et al.2 proposed diagnostic criteria for MIRM, which include: 1) <10% body surface area skin detachment; 2) involvement of two or more mucosal sites; 3) limited vesiculobullous or targetoid skin lesions; and 4) confirmed MP infection via IgM serology or PCR.2 Recent recognition of MIRM has led to updates in diagnostic and therapeutic recommendations. A 2023 systematic review highlighted the broad spectrum of MP-related extrapulmonary complications, including MIRM. MIRM represents one of the most clinically significant extrapulmonary presentations, often mimicking other mucocutaneous disorders (e.g., SJS). This review emphasised the diagnostic complexity of atypical presentations (e.g., isolated mucositis without rash or pneumoniae).13 In parallel, the 2022 international consensus guidelines defined refined diagnostic parameters for MIRM, emphasising the importance of laboratory confirmation (e.g., PCR) and the exclusion of drug- induced aetiologies.4
Treatment remains primarily supportive. While systemic corticosteroids, IV Ig, plasmapheresis, and TNF-α inhibitors have been used, data supporting their routine use are limited.7,14 Most patients respond well to macrolides such as azithromycin or clarithromycin, although there are reports of relapses or inadequate responses.14,15
Generally, MIRM has a favourable prognosis, with complete resolution reported in 81% of patients. However, approximately 11% may experience mucosal sequelae such as pigmentary changes (hyperpigmentation), synechiae, and recurrent pseudomembranous conjunctivitis or ulceration. A systematic review analysed 119 cases of MIRM and found that approximately 81% of patients achieved full recovery without long-term complications.16 This strengthens the evidence supporting the treatment response observed in the authors’ case.
The remaining cases exhibited varying degrees of residual effects, such as skin scarring or ocular sequelae (recurrent pseudomembranous or conjunctival ulceration).13 One case report described severe complications, including herpes simplex virus dissemination and bacteraemia (e.g., Staphylococcus epidermidis), highlighting the need for vigilant follow-up.12
CONCLUSION
This case has a few limitations. The authors conclude that a mucosal biopsy could have given a histopathological correlation, but it was postponed because of rapid clinical improvement. Furthermore, the use of metronidazole and nystatin, while clinically justified, might have complicated the evaluation of azithromycin’s effectiveness. This article reports on the potential impact on patient care, scientific integrity, and the inclusion of pertinent information intended to evoke critical inquiry and further investigation into MIRM, which serves to enrich discourse and deepen understanding within the field.






