INTRODUCTION
The classic triad of renal cell carcinoma (flank pain, haematuria, and a palpable abdominal mass) is observed in only 9% of patients. When present, it strongly suggests locally advanced disease.1,2 Further radiological imaging in patients presenting with haematuria and flank pain can improve surgical outcomes. This report presents a nephrectomy case involving a locally invasive kidney mass, thrombus in major vessels, and the rare anomaly of the left common iliac vein draining into the left renal vein.
CASE REPORT
A 48-year-old male patient with a known history of hypertension presented with a 1-week history of flank pain and macroscopic haematuria. Contrast-enhanced CT angiography of the abdomen showed a mass approximately 9 cm in size, occupying almost the entire left kidney. The left renal vein was dilated, with a tumour thrombus filling the lumen and extending to the suprarenal level into the inferior vena cava (Figure 1). Additionally, it was noted that the left common iliac vein was draining into the left renal vein, and a thrombus was also found in the iliac vein beyond the level where it joined the renal vein. A cystoscopy was performed to check for bladder involvement, which was negative for a tumour. Following this, a midline abdominal incision was made. After medialisation of the colon, the retroperitoneal space was accessed. A 9 cm mass was palpated in the left kidney, and dissection began. Due to the mass’s vascularity and surrounding tissue reaction, dissection was challenging. After completing dissection at the posterior kidney, superior dissection was done, and the left renal vein and its connection with the left common iliac vein were exposed and suspended. The cardiac and vascular surgery team was consulted. The renal artery was clamped, transected, and sutured. Both the left common iliac vein and inferior vena cava were clamped, and an incision was made over the common iliac vein. The tumour thrombus filling both the renal and iliac veins was visualised, dissected from the vein wall, and removed. The left common iliac vein was repaired with a 6-0 Prolene (Ethicon Inc, Raritan, New Jersey, USA) suture. After the clamp was released, no further bleeding was observed, and nephrectomy was completed. Lymph node dissection was performed in the paracaval and parailiac regions. A silicone drain was placed in the surgical area, and the incision was closed in layers.
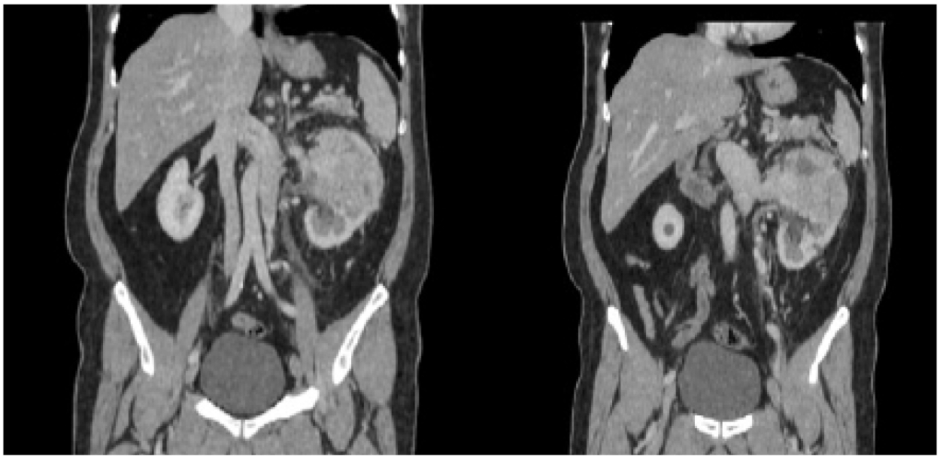
Figure 1: Contrast-enhanced CT angiography of the abdomen.
The patient was monitored in the ICU for 1 day post-operatively and was discharged on the seventh post-operative day without complications. The patient has been followed by medical oncology for 2 years for lung metastases, which have shown signs of regression since the initial presentation.
DISCUSSION
The typical course of the left renal vein is posterior to the superior mesenteric artery, anterior to the aorta, and cranial to the inferior mesenteric artery, where it drains into the inferior vena cava.3 There are several reports of variations in the drainage of the left renal vein. Common variants include retroaortic and circumaortic left renal veins. The incidence of these variants has been reported as 0.5–3.1% and 0.02%, respectively.4 In this case, the left common iliac vein drained into the left renal vein, which in turn drained into the inferior vena cava. A review of the literature revealed no previous reports of a similar vascular anomaly.
CONCLUSION
Iliac and renal vascular variants are not uncommon and may pose a risk for injury during retroperitoneal surgery. Failure to recognise these variants can lead to vascular damage and significant haemorrhage. In this case, awareness of this rare vascular variation preoperatively and intraoperatively allowed for safe conduct of the surgery.





