Interview Summary
Erectile dysfunction (ED) is a prevalent condition that extends beyond physical symptoms, serving as a critical marker for overall male health and significantly impacting quality of life (QoL). In this interview, conducted by EMJ, Sam Ward, a urologist at Saint Jean Clinic in Brussels, Belgium; and United Nations Educational, Scientific and Cultural Organization (UNESCO) Co-Chair in Sexual Health and Human Rights, explores the multifactorial nature of ED and the persistent psychological and societal barriers to treatment. Ward discusses the importance of normalising sexual health conversations, involving partners, and leveraging telemedicine to overcome embarrassment. He highlights the key role of phosphodiesterase Type 5 (PDE5) inhibitors as the cornerstone of pharmacotherapy, advocating for a personalised “and/and” approach rather than a rigid choice between agents. The discussion also explores the emergence of sildenafil orodispersible film (ODF), specifically how this formulation may suit the lifestyle needs of patients. Finally, Ward underscores the vital link between ED and cardiovascular (CV) health, urging clinicians to view ED as a window into a patient’s systemic well-being.INTRODUCTION
ED is classically defined as the persistent inability to attain and/or maintain an erection sufficient for satisfactory sexual performance.Contemporary guidelines describe it not as a single disease or localised disorder but as a symptom with multifactorial aetiologies, ranging from vascular and neurogenic causes to hormonal, psychological, and medication-related factors.1,2
Epidemiological data, including the landmark Massachusetts Male Aging Study, illustrate a strong correlation between increasing age and ED prevalence, with up to 70% of men affected by age 70.3,4 Further epidemiological studies from European and global cohorts suggest that moderate-to-severe ED affects roughly 5–20% of men, with prevalence correlating strongly with age and cardiometabolic comorbidity.5 One in four patients seeking help for new-onset ED are below the age of 40 years, with almost 50% of these young men complaining of severe ED.2 Beyond the statistics, the condition carries a profound burden on QoL.4 “ED has a negative effect on self-esteem, mood, masculinity, and relationship satisfaction,” Ward explained, adding that ED impacts three key QoL pillars: “general QoL, sexual satisfaction, and mental health.” Men often report avoiding intimacy or withdrawing from relationships, leading partners to experience rejection and anxiety about the couple’s future.6-8 Conversely, successful treatment has been shown to improve not only ED but also broader QoL, relationship indices, and mental health for both partners in a couple.9
WHY DOES ERECTILE DYSFUNCTION REMAIN A SENSITIVE OR TABOO TOPIC?
Despite its high prevalence, Ward explained that ED remains shrouded in stigma, deeply entwined with cultural scripts surrounding virility and ageing. Many men equate erectile capacity with their identity and self-worth; therefore, losing this function can be experienced as a diminished sense of manhood. Sexuality in later life can also be minimised, with the assumption that sex is less important to older people, and seeking help is often viewed as shameful.10
Ward highlighted that psychological barriers, such as embarrassment, fear of judgment, and anticipatory anxiety about sexual performance, are frequent. “Partners may avoid raising the issue for fear of hurting the man’s feelings, which creates a vicious circle and reinforces the silence,” he noted. Studies on PDE5 inhibitors have shown that non-initiation and discontinuation are often driven by psychosocial factors, such as unrealistic expectations, anxiety, relationship conflict, and lack of communication, more than by pharmacological failure alone.11 Furthermore, while patient-focused communication has increased awareness, it has inadvertently fostered unrealistic expectations that ED is a purely mechanical issue to be “fixed by a pill.”12
HOW CAN CLINICIANS ENCOURAGE OPEN DISCUSSIONS AND INVOLVE THE PARTNER?
To dismantle these barriers, Ward emphasised the necessity of firstly normalising the language used in clinical settings. He advocated for routine, matter-of-fact inquiries about sexual function, treating ED as a common and important medical condition rather than a sexual failure. “I ask routinely about sexual health in all discussions with all my patients, even if they present for other symptoms like prostate or bladder issues,” Ward stated. “It sends the message that this is a legitimate medical condition.”
Strategies that help include training in structured sexual history taking and the use of validated tools like the International Index of Erectile Function (IIEF).13 Involving the partner is also a critical strategy. Evidence from couple-based trials suggests that partner engagement is associated with higher treatment concordance and satisfaction.9 Ward advised clinicians to explicitly invite partners to share their perspectives, thereby reframing ED as a couple’s issue to be addressed collaboratively. European Association of Urology (EAU) guidelines also emphasise psychosocial assessment and, when indicated, referral for psychosexual therapy.2
WHAT ROLE DO TELECONSULTATIONS PLAY IN REDUCING EMBARRASSMENT?
The rise of telemedicine has been a “game changer” for sexual medicine, particularly in reducing the embarrassment associated with face-to-face consultations.14 As Ward explained, digital platforms allow patients to discuss intimate issues from the comfort of their own homes, which can be particularly encouraging for younger men who might otherwise delay seeking help. “Eighteen months is the average time it typically takes for patients to open up about ED,” noted Ward.15 In an ecological study of over 600 men, median time to seeking first medical help for new-onset ED was around 12 months, with a mean of approximately 30 months.15
“Studies in sexual medicine practices during and after COVID-19 show that telemedicine improves access and reduces the travel burden, reduces the embarrassment of discussing intimate issues face-to-face in a crowded hospital, and facilitates partner participation,” Ward observed.14 This format allows younger or tech-savvy patients to seek help earlier, sometimes via patient-focused ED platforms that emphasise discretion. However, he cautioned that telemedicine should function as an adjunct to, rather than a replacement for, comprehensive in-person care. Physical examinations remain necessary in many cases to rule out underlying pathologies, for CV risk stratification and holistic assessment, and to ensure that the convenience of digital access does not lead to over-simplified pill-only management, Ward stressed.
WHAT ARE THE MAIN MEDICAL TREATMENTS FOR ERECTILE DYSFUNCTION, AND HOW IS THE DECISION MADE IN CLINICAL PRACTICE?
First-line therapy for ED combines lifestyle optimisation and comorbidity management, with evidence-based pharmacotherapy. PDE5 inhibitors are the current therapeutic cornerstone.1,2,16
In clinical practice, the choice between agents is based on patients’ specific needs regarding onset, duration, and frequency of sexual activity. Sildenafil offers a short-acting, on-demand profile, while tadalafil provides a longer duration of action.17 Ward argued against a binary choice: “For me, it is not an ‘or/or’ story, but an ‘and/and’ story. Both options are needed, and we should adapt the tablet to the moment the patient is in.” The decision-making process should also factor in comorbidities and drug interactions, such as concurrent use of nitrates or severe cardiac disease, as well as the aetiology and severity of the ED (e.g., higher doses post-prostatectomy), he advised. It is also important to consider patient preference regarding timing, frequency of dosing, and side-effect profile.
Crucially, Ward stressed the importance of managing patient expectations and aligning these with realistic goals. Clinicians must educate patients that PDE5 inhibitors are not a “cure,” and facilitate erections in response to sexual stimulation, but do not initiate them.18 “I tell patients that the first time they take a tablet, it might not work, simply due to the mental tension and pressure,” he said. “The goal is usually sufficient rigidity for satisfactory intercourse most of the time, rather than perfection every time.”
Ward explained that dose titration, switching agents or regimens, and addressing relationship conflicts are essential steps to prevent premature discontinuation, which affects nearly half of all users.1,2,19,20 “Studies on PDE5 discontinuation show that unmet expectations and poor education are major reasons for dropout,” he emphasised.
HOW DOES THE SILDENAFIL ORODISPERSIBLE FILM MEET THE LIFESTYLE NEEDS OF PATIENTS?
A significant development in the ED treatment landscape has been the introduction of sildenafil ODF.21 “PDE5 inhibitors like sildenafil have now been on the market for over 25 years, so we understand them exceptionally well,” Ward reflected.22 “Their efficacy is predictable, their side-effect profile is well-characterised, and millions of men globally have used them safely.22 What is really changing today is not the pharmacology, but the experience men have with their treatment.”
“There is also a strong element of trust here,” Ward added. “Sildenafil is a medication that men openly recognise; they know friends who use it, and they’ve seen it discussed in culture and media. It has become part of the social understanding of men’s health. When you combine that deep trust in safety and outcomes with formats that respect modern sexual life, mobility, spontaneity, and privacy, we are not just treating ED, we are improving QoL, confidence, and relationship well-being.”
HOW DOES RELATIONSHIP STATUS AND AGE INFLUENCE PREFERENCE FOR ORODISPERSIBLE FILMS?
“The ODF formulation aligns well with the needs of younger patients on several fronts,” Ward explained.23-25 “First, there is discretion and portability.23-25 The film is incredibly thin and easy to carry in a wallet, which is attractive in social settings or casual encounters where a patient might not want to be seen taking medication.”23-25 The rapid dissolution without water also supports spontaneity, he added.23-25 Real-world data support these clinical observations. Observational studies with sildenafil ODF have reported good acceptance in younger cohorts and significant improvements in sexual QoL.26,27
However, Ward pointed out that this formulation is not exclusively for the young. It is also a valuable option for older patients with dysphagia, polypharmacy (minimising pill burden), and those with a desire for subtlety in family settings. “Ultimately, it is about offering options,” Ward concluded. “A formulation that addresses lifestyle needs can improve satisfaction and reduce the dropout rates we often see with traditional therapy.”
WHEN MIGHT ORODISPERSIBLE FILM FORMULATIONS BE PREFERABLE TO FILM-COATED TABLETS?
Ward emphasised that the pharmaceutical industry has shifted from simply providing a tablet to delivering solutions that better fit into men’s everyday lifestyles. Developed to address practical limitations of traditional film-coated tablets, such as swallowing difficulties, aversion to pills, and the need for water, ODF formulations offer a discreet and convenient alternative (Table 1).21 Ward noted that for many patients, the physical act of taking a pill can reinforce a sense of “being sick,” whereas a film that dissolves on the tongue feels less “medicalised” and more natural.
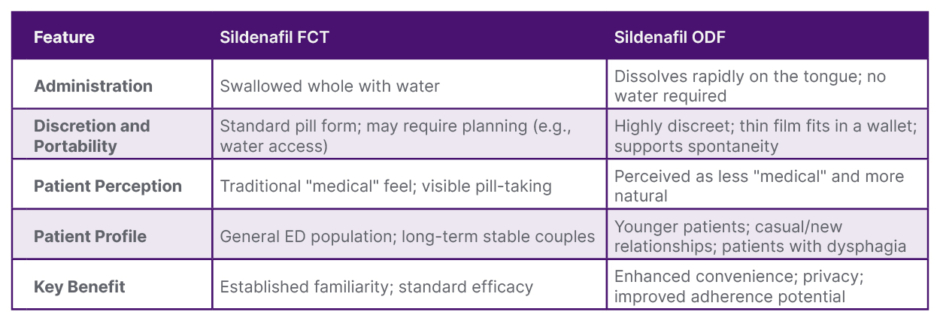
Table 1: Comparison of sildenafil formulations: film-coated tablets versus orodispersible film.21
Adapted from Cocci A et al.21 and interview insights.
ED: erectile dysfunction; FCT: film-coated tablet; ODF: orodispersible film.
Head-to-head and observational data show that sildenafil ODF is non-inferior in efficacy to conventional tablets, with advantages in convenience and discretion.21,27,28 In particular, Ward explained that ODF formulations may be preferable when the patient has swallowing difficulties or aversion to tablets, discretion is important, or a more “on-the-go” format is desired.
Beyond convenience, Ward highlighted the sensory advantages of the ODF formulation. “Patients often tell me: ‘I put it on my tongue, and it works very easily’. The perception of a faster onset, even if pharmacokinetics are comparable to tablets, is a powerful psychological benefit,” he said. “The mint taste is also well-accepted, adding to a positive treatment experience.” This aligns with recent trends in pharmaceutical development, focusing on optimising the patient experience to improve long-term adherence.
WHY IS ERECTILE DYSFUNCTION CONSIDERED A MARKER OF SYSTEMIC HEALTH AND CARDIOVASCULAR RISK?
Beyond sexual function, Ward underscored the critical role of ED as a barometer for systemic health, specifically CV well-being. The “artery size hypothesis” posits that because penile arteries are smaller than coronary arteries, they are more susceptible to occlusion by atherosclerotic plaques (Figure 1).29,30 Consequently, ED often precedes symptoms of coronary artery disease by 2–3 years and major CV events by 3–5 years.29,30 Severe ED (as denoted by lower IIEF scores) has also been shown to correlate with higher Charlson Comorbidity Index (CCI) scores, further supporting ED as a proxy for general health.29
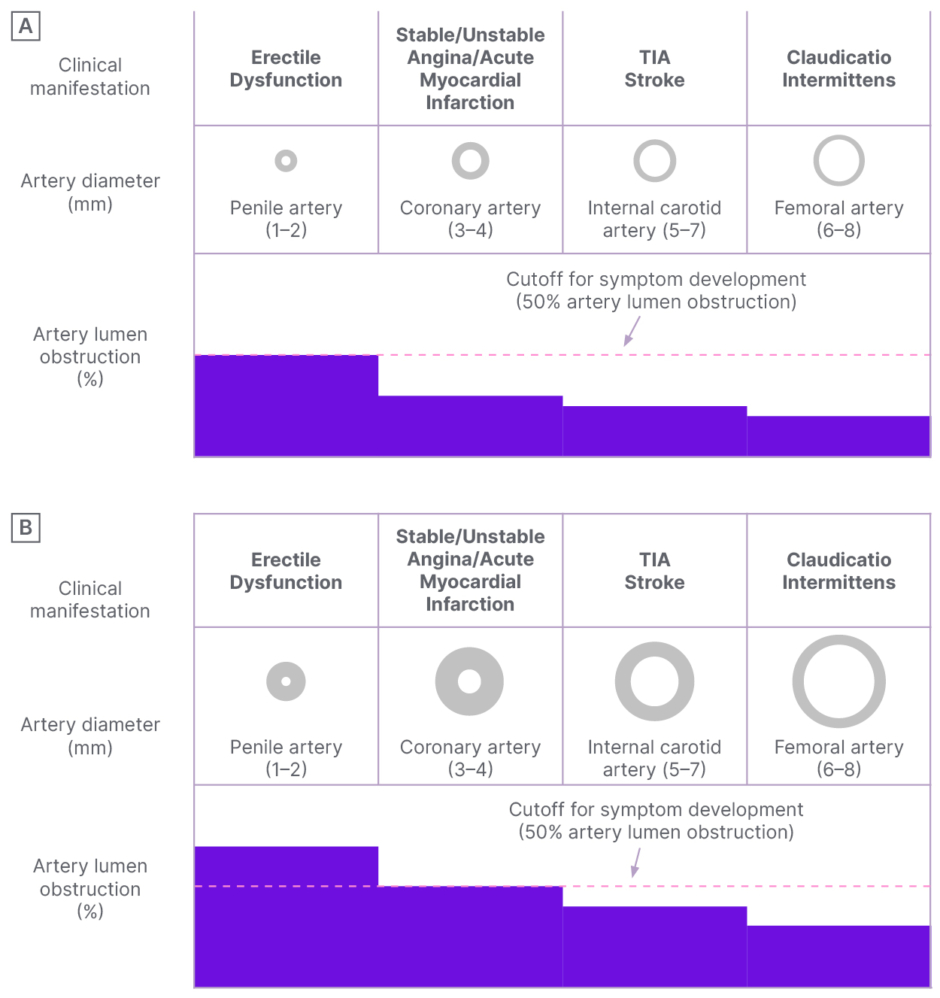
Figure 1: The artery size hypothesis.30
A) Early stage of the atherosclerotic process. Significant vascular obstruction (>50% lumen artery narrowing) of penile circulation leading to erectile dysfunction symptoms is shown. B) Late stage of the atherosclerotic process. Significant vascular obstruction of coronary circulation leading to angina pectoris is shown.
TIA: transient ischaemic attack.
“Erectile health is the mirror of general health,” Ward asserted. “Risk factors for coronary artery disease, diabetes, hypertension, smoking, and obesity are the same for ED.”2,31 This correlation makes the urologist or sexual medicine specialist a front-line defender in preventative health. EAU guidelines now recommend that a diagnosis of ED, particularly in younger men without known CV disease, should prompt a comprehensive CV risk assessment.1,2,32
WHAT IS THE MOST IMPORTANT TAKEAWAY FOR CLINICIANS?
Ward encouraged clinicians to view ED not just as a sexual complaint but as a gateway to broader health management. The key to optimising outcomes lies in normalising the conversation, involving partners early, and tailoring pharmacotherapy to the individual’s lifestyle, whether that means leveraging the discretion of ODFs or ensuring spontaneity with longer-acting agents. “I try to model comfort and neutrality, avoid assumptions about orientation or relationship style, and make it explicit that any sexual concern is legitimate medical business,” Ward advised. Crucially, a diagnosis of ED should trigger a comprehensive CV risk assessment, positioning the clinician at the forefront of preventative care. Appropriate training, use of validated tools and telemedicine, and interdisciplinary collaboration are all key to success. By integrating these strategies with a supportive, non-judgemental approach, practitioners can overcome barriers to ED treatment and improve long-term adherence.
| Adverse events in the UK can be reported on 00441707 853000 (select option 5) or at [email protected]. Adverse events should be reported to Viatris via the country-specific information at https://www.viatrisconnect.com/en/viatris-ae. |





