Abstract
Background: Focal fatty sparing (FFS) is a benign, localised absence of hepatic fat in an otherwise steatotic liver, frequently identified on surveillance liver ultrasound in patients with advanced chronic liver disease (ACLD). However, FFS can mimic hepatocellular carcinoma (HCC), and may prompt clinicians to further investigate with cross-sectional imaging, such as CT or MRI.
Aim: This study aimed to assess the incidence of HCC in patients with ACLD with newly identified FFS on surveillance ultrasound, evaluate radiographic concordance between ultrasound and cross-sectional imaging, and describe associated demographic and metabolic characteristics.
Methods: The authors retrospectively identified 53 patients with ACLD with new FFS detected during routine liver ultrasound, under a nurse-led HCC surveillance programme, between January 2016–December 2024. Inclusion criteria included liver stiffness measurement ≥10 kPa or nodular liver contour on ultrasound. Clinical data, ACLD aetiology, metabolic risk factors, alpha fetoprotein (AFP) levels, and follow-up imaging (CT/MRI) were analysed.
Results: A total of 445 patients were screened, and 53 patients were identified for analysis. The median age was 60 years (range: 37–83 years), 67.9% were male, and most had MASLD (41.5%) or mixed aetiologies (43.4%). The median AFP was 3.3 IU/mL (range: 0–10), and the median BMI was 31.7 kg/m2. Type 2 diabetes, dyslipidaemia, and hypertension were present in 28 (52.8%), 27 (50.9%), and 22 (41.5%) patients, respectively. Multiple liver-related risk factors were observed in 37 (69.8%) patients. Cross-sectional imaging was performed in 38 (71.7%) patients, with concordant FFS findings in eight (21.1%; 95% CI: 9.6–37.3). No HCC cases were diagnosed. Fifteen patients did not undergo subsequent cross-sectional imaging as per clinician’s decision. Instead, they resumed routine 6-monthly HCC surveillance with a median follow-up duration of 25 months (range: 7–112 months) and no HCC cases were diagnosed.
Conclusion: New FFS on surveillance ultrasound in patients with ACLD was not associated with increased risk of HCC. Routine escalation to CT or MRI imaging may be more appropriate in the presence of high-risk features such as lesion size ≥10 mm, nodularity, or elevated AFP. This approach could reduce patient harm through radiation exposure and reduce healthcare costs, emphasising the need for a standardised diagnostic pathway.
Key Points
1. In patients with advanced chronic liver disease undergoing hepatocellular carcinoma (HCC) surveillance, newly detected focal fatty sparing (FFS) on ultrasound often prompts escalation to cross-sectional imaging. These findings show that FFS was not associated with HCC, challenging the assumption that new FFS invariably warrants cross-sectional imaging.2.In a single-centre retrospective cohort of 53 patients with advanced chronic liver disease and newly detected FFS on surveillance ultrasound, 71.7% underwent CT or MRI. Concordant FFS was confirmed in only 21.1% of cases, and no HCC diagnoses were made during a median follow-up of 25 months.
3.These data support a risk-stratified approach, reserving CT or MRI for high-risk lesions, such as lesions ≥10 mm in size, with suspicious morphology or elevated alpha fetoprotein, in line with international guidance. Selective imaging may minimise unnecessary radiation exposure, contrast risk, incidental findings, and healthcare costs, while maintaining safe HCC surveillance in this high-risk population.
INTRODUCTION
Focal fatty sparing (FFS) is characterised by localised regions within the liver with an absence of fat infiltration, appearing as hypoechoic or isoattenuating areas on imaging amidst a diffusely steatotic liver.1,2 It typically occurs in predictable anatomical locations such as the gallbladder and hepatic hilum, influenced by directed splanchnic venous supply to the liver other than portal venous flow.3
Although benign, FFS can mimic true focal liver lesions, raising concern for hepatocellular carcinoma (HCC) or metastasis. The differentiation of such focal spared areas from true tumours has been a diagnostic challenge, as ultrasound alone cannot always reliably distinguish FFS from a tumour.
The distinction is clinically significant in patients with advanced chronic liver disease (ACLD), where the annual HCC risk is approximately 2.4%.4 Surveillance for HCC in ACLD commonly relies on liver ultrasound and serum alpha fetoprotein (AFP) every 6 months.5 Newly detected FFS may prompt clinicians to further investigate with cross-sectional imaging, such as liver multiphase CT or liver MRI. However, this practice poses risks of radiation exposure, contrast-related risks, incidental findings, and healthcare resource utilisation.
Despite the clinical relevance of FFS in HCC surveillance, there is a lack of literature evaluating the outcomes of FFS detection in patients with ACLD undergoing surveillance. To the authors’ knowledge, this represents the first study to systematically examine the incidence of HCC and the diagnostic utility of cross-sectional imaging following newly identified FFS in a dedicated HCC surveillance cohort. This evidence gap has growing relevance in contemporary hepatology practice given the rising prevalence of metabolic liver disease.
This study aimed to evaluate the incidence of HCC in patients with ACLD with new FFS detected on surveillance ultrasound, assess concordance with cross-sectional imaging findings, and describe associated demographic and metabolic characteristics of this population.
METHODS
A retrospective observational cohort study was conducted at Gold Coast University Hospital, Queensland, Australia. The Gold Coast Hospital and Health Service Research Office deemed the study as not requiring HREC review. For publication purposes, the HREC reference is EX/2024/QGC/114893.
Patients with ACLD enrolled in a nurse-led HCC surveillance programme from January 2016–December 2024 were screened. Eligibility criteria included newly detected FFS on routine surveillance liver ultrasound in patients with confirmed ACLD. Exclusion criteria included patients under the age of 18 years, those without a confirmed diagnosis of ACLD, pre-existing or previously diagnosed HCC, and prior liver transplantation. ACLD was defined according to the Baveno VII consensus guidelines, using a liver stiffness measurement (LSM) ≥10 kPa on Fibroscan or nodular liver contour on ultrasound where LSM was inconclusive.6,7 ACLD aetiologies were classified in accordance with current nomenclature guidelines as alcohol-related liver disease, MASLD, chronic viral hepatitis B or C, or mixed aetiology. Mixed aetiology was defined as the co-existence of two or more contributing aetiologies, most notably MASLD combined with alcohol-related liver disease or chronic hepatitis.
FFS was defined as a hypoechoic, solid, avascular focus within a background of diffusely hyperechoic liver parenchyma irrespective of hepatic location. Lesion size was not included as the sizing was inconsistently stated across reports. Ultrasound findings were retrospectively documented from imaging reports. Demographic data, ACLD aetiology, metabolic risk factors (Type 2 diabetes, dyslipidaemia, hypertension), serum AFP, LSM values, and ultrasound findings were retrospectively extracted from electronic medical records. CT or MRI performed after FFS detection was reviewed for concordance and presence of HCC. The primary outcome was the diagnosis of HCC following newly detected FFS on ultrasound. The secondary outcome was HCC detection on longitudinal follow up until July 2025 among patients who did not undergo cross-sectional imaging. Continuous variables are reported as median with range. Categorical variables are expressed as frequencies and proportions. The primary outcome is reported with 95% CI using the frequentist framework method. Given the observational nature of the study and the sample size of 53 patients, no formal power calculation was performed.
RESULTS
Of 445 screened patients, 53 met inclusion criteria. Median age was 60 years (range: 37–83 years), with 36 males (67.9%). The majority had MASLD (41.5%) or mixed aetiology (43.4%). Median LSM was 13.6 kPa, median AFP was 3.3 IU/mL, and median BMI was 31.7 kg/m². Two patients did not have an LSM recorded but met inclusion criteria due to presence of a nodular liver contour on liver ultrasound. Metabolic comorbidities were frequent, including Type 2 diabetes (52.8%), dyslipidaemia (50.9%), and hypertension (41.5%). Nearly 70% had two or more of the listed metabolic risk factors for liver disease. Cross-sectional imaging was performed in 38 (71.7%) patients. Concordant FFS findings on CT or MRI were identified in eight (21.1%; 95% CI: 9.6–37.3) cases. No patients were diagnosed with HCC during the study period. Of the 38 patients who underwent cross-sectional imaging, five had incidental findings that required further investigations. The 15 patients who did not undergo further imaging continued routine 6-monthly ultrasound surveillance without detection of a focal liver lesion. These patients were followed longitudinally until July 2025, with a median follow-up duration of 25 months (range: 7–112 months). No HCC diagnoses were made in this subgroup during follow-up (Table 1).
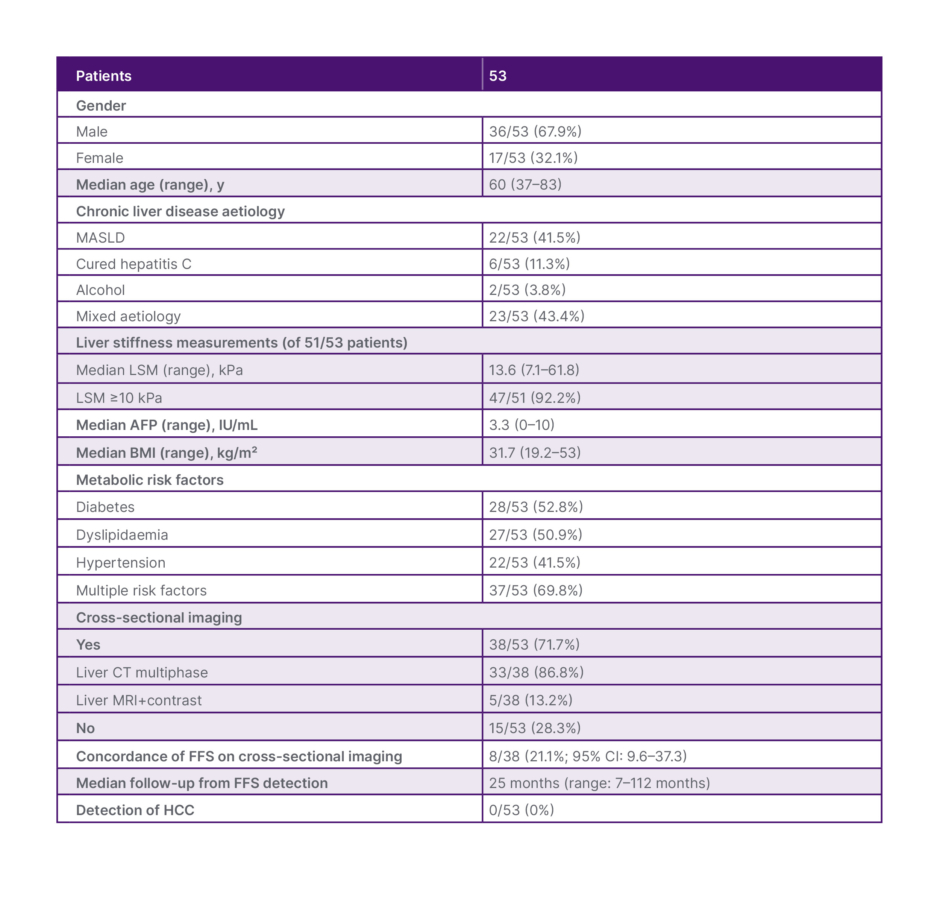
Table 1: Patient demographics and imaging data.
AFP: alpha fetoprotein; FFS: focal fatty sparing; HCC: hepatocellular carcinoma; LSM: liver stiffness measurement; MASLD: metabolic dysfunction-associated steatotic liver disease.
DISCUSSION
Newly detected FFS on ultrasound can mimic a true focal mass and may raise concern for HCC in patients with ACLD.8,9 In the authors’ cohort, 71.7% of newly detected FFS lesions were further investigated with cross-sectional imaging, reflecting a common clinical practice to escalate to CT or MRI when faced with indeterminate findings on ultrasound. In this healthcare setting, there were no barriers to accessing cross sectional imaging when clinically indicated.
Imaging concordance between ultrasound and cross-sectional imaging was limited, with FFS confirmed in 21.1% (95% CI: 9.6–37.3%) of cases. However, this should not be interpreted as evidence of poor ultrasound sensitivity or diagnostic inaccuracy. The two imaging modalities detect hepatic fat through different physical principles. Ultrasound identifies FFS as a relative hypoechogenicity against a hyperechoic steatotic background, whereas cross-sectional imaging relies on attenuation differences for CT or chemical-shift signal dropout for MRI.10 Therefore, FFS that is sonographically apparent may not meet quantitative thresholds for detection on cross-sectional imaging, particularly when background steatosis is mild. Discordance between modalities likely reflects differences in the technique sensitivity for detecting subtle parenchymal fat variation rather than ultrasound inaccuracy. The possibility that some non-concordant cases represented genuine FFS below the detection threshold of CT or MRI cannot therefore be excluded.
In the authors’ cohort, no HCC diagnoses were made, suggesting that routine escalation to CT or MRI in the absence of high-risk features may not always be warranted. This is consistent with current American Association for the Study of Liver Diseases (AASLD) and European Association for the Study of the Liver (EASL) guidance, which recommend diagnostic CT or MRI for any new nodule ≥10 mm, nodules with suspicious morphology, or when accompanied by an elevated or rising AFP, while lesions <10 mm without high-risk features are typically managed with short interval repeat ultrasound.5,11 However, this must be interpreted with caution, given the retrospective single-centre design, small sample size, and absence of a comparator group.
The decision to pursue to cross-sectional imaging, while invaluable for diagnosis, exposes patients to ionising radiation and carries risks of contrast-related adverse events for CT, whereas MRI avoids radiation but remains costly and may still pose contrast-related risks.12 Cross-sectional imaging may reveal incidental findings that can trigger a cascade effect of care. In the authors’ study, five incidental findings were identified, none of which resulted in a new clinically significant diagnosis, yet each prompted further imaging and potentially invasive investigations. This illustrates how incidental findings can lead to increased healthcare costs and a considerable psychological burden for patients, without improving outcomes.13
Several limitations warrant acknowledgement. The retrospective design introduced selection and ascertainment bias. Patients were included only if FFS was identified and reported, and the decision to proceed with cross-sectional imaging was clinician dependent rather than protocol driven. Patients who did not undergo cross-sectional imaging may have represented a clinically lower-risk subgroup, and the absence of HCC in this group should be interpreted in that context. Ultrasound detection of FFS is further influenced by degree of background steatosis, operator experience, equipment quality, and patient habitus, suggesting the true prevalence of FFS in ACLD surveillance populations is likely underestimated.14,15
Although limited by its retrospective single-centre design and small sample size, this study represents the first focused investigation of FFS in a cohort with ACLD undergoing HCC surveillance. It provides valuable clinical insights into the frequency of cross-sectional imaging escalation, the complexity of intermodality concordance on imaging, and the consequences of incidental findings. This study offers a foundation upon which prospective, multicentre studies can be designed to better define the optimal HCC surveillance and investigation pathway for this population.
In this cohort of patients with ACLD undergoing HCC surveillance, no HCC was diagnosed following newly detected FFS on liver ultrasound, and concordance with cross-sectional imaging was limited. These findings support a more selective, risk-stratified imaging strategy consistent with currently AASLD and EASL guidance, with the potential to reduce radiation exposure, contrast-related risks, and healthcare resource use. To the authors’ knowledge, this is the first study to systematically examine HCC incidence and cross-sectional imaging utility following newly detected FFS in a dedicated HCC surveillance cohort. Prospective multicentre studies with standardised imaging protocols and longer follow-up are needed before definitive recommendations can be made.





