INTRODUCTION
Preparedness for high-consequence infectious diseases (HCID) does not begin when a patient is placed in isolation. It begins much earlier, with awareness: knowing what is circulating globally, where outbreaks are evolving, and how that information should shape frontline screening, infection prevention, and operational response. In a world defined by rapid travel, dense cities, and increasingly frequent outbreaks, that awareness is no longer optional. It is foundational. Recent events underscore this reality: in May 2026, a multi-country hantavirus cluster linked to cruise ship travel prompted public health monitoring and quarantine actions, while Ebola outbreaks in the Democratic Republic of the Congo and Uganda reinforced how quickly high-consequence pathogens can create cross-border risk and operational pressure for health systems.
That is the rationale behind the new Special Pathogens Biopreparedness Map, an open-source initiative developed by NYC Health + Hospitals, New York, USA, and embedded within their website (Figure 1). The interactive map visualizes current outbreak activity to support clinicians, public health officials, and emergency management professionals in monitoring and responding to special pathogens and other biological threats. It was built to connect global epidemiology with local decision-making. By translating evolving outbreak signals into accessible situational awareness, the map helps users recognize when distant events may have local implications for screening, preparedness, and healthcare operations.
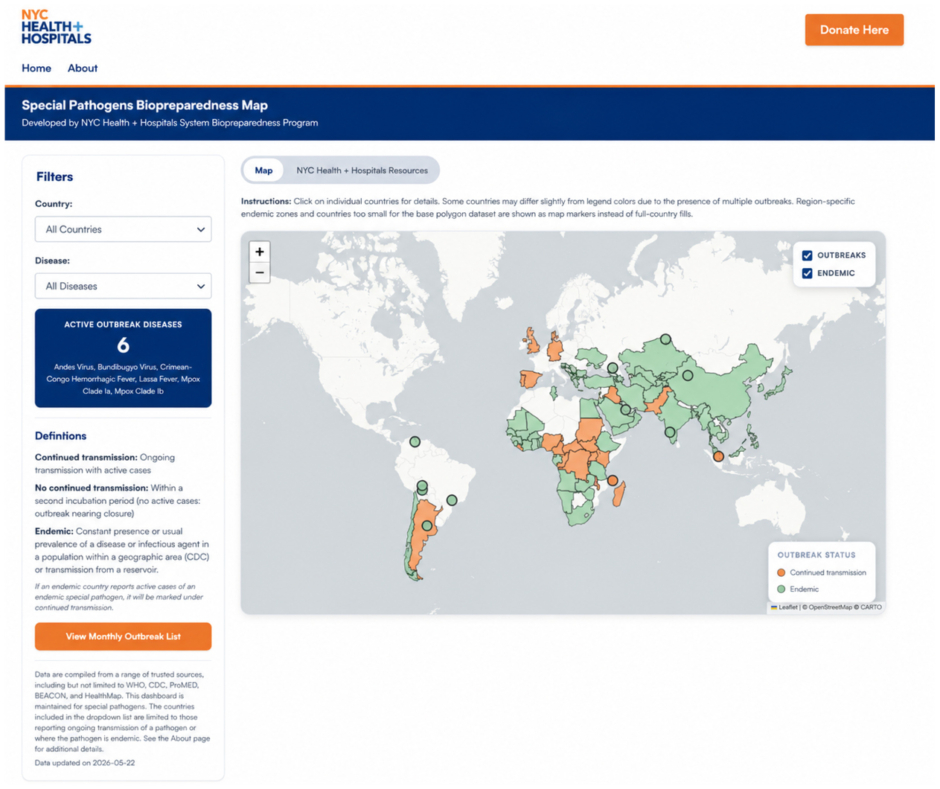
Figure 1: Special Pathogens Biopreparedness Map.
This connection matters because the earliest warning sign of a special pathogen is rarely a definitive diagnosis. It is often a fever in a returning traveler, an exposure history that raises concern, or a triage nurse recognizing that the clinical picture does not fit the usual pattern. In these moments, preparedness depends on whether frontline teams can rapidly identify possible risk, isolate appropriately, and inform the right people. That operational logic is well captured by the longstanding “Identify, Isolate, and Inform” CDC framework, which remains central to the frontline management and outbreak prevention of any pathogenic microbes, especially HCIDs.¹
WHAT ARE SPECIAL PATHOGENS?
The term “special pathogens” is used to describe infectious agents that require enhanced clinical, infection prevention, and operational attention. According to a published frontline planning guide,2 these pathogens are associated with high morbidity and/or mortality, may have a high likelihood of secondary transmission, often lack effective vaccines, prophylaxis, or treatment, and may prompt the use of biocontainment because of clinical or public health concerns.2 In practical terms, these are pathogens that pose a substantial risk to healthcare personnel and require rapid identification, prompt isolation, and disciplined infection control.
Examples include Ebola disease, Marburg virus disease, Lassa fever, and other emerging or high-consequence pathogens that can quickly expose weaknesses in routine clinical workflows. Beyond their direct clinical consequences, HCIDs can also disrupt healthcare delivery, including emergency department operations, staffing, patient volumes, and elective care. The 2014 U.S. Ebola experience demonstrated this clearly: while Emory University Hospital’s (Atlanta, Georgia, USA) preparedness supported safe care, Texas Health Presbyterian Hospital Dallas, USA, experienced major operational and reputational fallout, including a 25% revenue decline and a 50% drop in emergency department visits, underscoring the importance of preparedness, situational awareness, and timely risk communication.3
While not every pathogen displayed on the Special Pathogens Biopreparedness Map is formally categorized as a “special pathogen,” the purpose of the tool is broader: to improve situational awareness around infectious threats that could affect healthcare delivery and public health operations.
This distinction is important. Preparedness for special pathogens is often misunderstood as a niche exercise reserved for rare diseases or specialized units. In reality, it is a systems function. It requires emergency departments, infection prevention and control, emergency management, inpatient units, laboratory teams, emergency medical services partners, and public health agencies to work from a shared operational picture. The same disciplines that support a response to a suspected Ebola case, screening, escalation, personal protective equipment readiness, communication, safe transport, and role clarity, also strengthen readiness for other biological threats.2
THE LAST 5 YEARS HAVE MADE THE CASE
The need for this kind of preparedness is not theoretical. Over the last 5 years, the world has repeatedly faced outbreaks of special pathogens that underscore the continued risk of importation, delayed recognition, and operational strain. Since 2020, there have been seven documented Marburg outbreaks (three of which were the country’s first Marburg outbreak) and 10 documented Ebola disease outbreaks. In comparison, the previous 5 years (2014–2019) had two Marburg and four Ebola disease outbreaks (11 outbreaks, counting two secondary outbreaks and five travel-associated cases from the large 2014 West Africa Ebola outbreak).4-7 These figures represent an acceleration in outbreak frequency and geographic spread, utilizing Marburg and Ebola virus disease as examples that reflect the need for sustained preparedness.
In 2022, Uganda experienced an outbreak of Sudan virus disease (Orthoebolavirus sudanense), which was especially concerning because licensed countermeasures for Ebola virus disease (Orthoebolavirus zairense) could not simply be assumed to apply. In 2025, Uganda again reported Sudan virus disease, including cases in Kampala, before the outbreak was declared over in April 2025.8 In May 2026, a new Ebola disease outbreak caused by Bundibugyo virus was reported in the Democratic Republic of the Congo and Uganda, adding urgency to this distinction because there are no approved vaccines or treatments for Bundibugyo virus disease. The outbreak has also been described as only the third known outbreak caused by the Bundibugyo virus, underscoring both its rarity and the operational uncertainty it creates. Together, the Sudan and Bundibugyo outbreaks highlight a shared gap in preparedness: the need to accelerate species-specific medical countermeasures for non-Zaire Ebola viruses before outbreaks occur.9 These events reinforced a central lesson: even within the umbrella term “Ebola,” the specifics matter operationally. Species, transmission dynamics, available countermeasures, and healthcare readiness all shape response.
In 2024, Rwanda reported its first-ever Marburg virus disease outbreak. The WHO described it as one of the largest Marburg outbreaks documented, with healthcare workers among those affected.10 That detail is especially important. Special pathogens are not only a threat to patients and communities; they are a direct threat to healthcare workers when systems are unprepared or recognition is delayed. In late 2025, Ethiopia reported its first-ever Marburg outbreak. Unlike the Rwanda outbreak, the Ethiopia outbreak was relatively small, with a total of 14 confirmed cases, three of which were healthcare workers, and was contained in less than 3 months.11 However, its proximity to the South Sudan border highlighted concerns for regional vulnerabilities. With frequent cross-border population movement and South Sudan’s fragile healthcare system and limited response capability, there was concern for the potential of facilitation in the international spread of cases.12 This highlights that localized outbreaks may quickly evolve into international health emergencies requiring global responses.
Lassa fever remains another major concern. Endemic in parts of West Africa, it continues to cause substantial annual burden, particularly in Nigeria, where outbreaks recur seasonally, and surveillance challenges remain significant. A recent peer-reviewed review of Lassa fever epidemiology in Nigeria highlights the continuing need for stronger surveillance, early detection, and sustained preparedness capacity.13 Although endemic diseases can become normalized in the global health conversation, they still pose acute operational risk when cases are imported into settings unfamiliar with them.
That point was illustrated clearly in the United States. In late 2024, Iowa reported a travel-associated fatal case of Lassa fever in a returning traveler from Liberia, leading to a multistate response that involved the monitoring of 180 contacts.14 There was no transmission in the United States, but that does not diminish the significance of the event. A single imported case of a high-consequence pathogen can trigger major clinical, infection prevention, laboratory, and public health activity.
The same principle was evident more than a decade earlier with Middle East respiratory syndrome coronavirus (MERS). In 2014, the United States identified its first two imported MERS cases, both in healthcare workers returning from Saudi Arabia.15 These cases did not result in wider community transmission, but they demonstrated how quickly a global outbreak can become a domestic operational issue. For hospitals, the key challenge is not only whether transmission occurs; it is whether the system is prepared to recognize and manage the possibility safely from the outset.
WHY A BIOPREPAREDNESS MAP MATTERS
The value of the Special Pathogens Biopreparedness Map lies in its ability to make outbreak intelligence useful at the point of care and in emergency planning. Many public health dashboards are informative, but not all are designed with frontline healthcare operations in mind. Clinicians and emergency managers need more than epidemiologic data. They need to know what that data means for screening, escalation, isolation, and communication.
The map supports this need by providing a routinely updated visualization of special pathogen activity. It highlights pathogens with ongoing transmission as well as endemic special pathogens, helping users maintain situational awareness of threats that may require enhanced clinical, infection prevention, and operational readiness. It links users to disease-specific clinician fact sheets that summarize case definitions, signs and symptoms, epidemiologic risk factors, infection prevention and control considerations, and relevant reporting pathways. That combination is what makes the tool operational rather than purely informational.
In effect, the map helps bridge one of the most persistent gaps in preparedness: the gap between global events and local action. Outbreaks are often reported in a way that is understandable to specialists but not immediately actionable for frontline clinicians. A returning traveler with fever may be the first and only clue that a health system is confronting a rare pathogen. If clinicians, infectious disease specialists, infection prevention teams, and emergency managers do not have an easy way to connect that patient to current global outbreak activity, the opportunity for rapid action can be lost.
This is especially important because healthcare systems are busy, fragmented, and often dealing with multiple competing threats at once. Tools that reduce cognitive burden and accelerate recognition are therefore not a luxury. They are part of resilience.
FROM OUTBREAKS TO OPERATIONS AT MASS GATHERINGS
One of the clearest cases of use for the map is mass gathering preparedness, including planning for the FIFA World Cup 2026. Large international events create a unique public health environment: high population density, international travel, multiple jurisdictions, intense media attention, and pressure on healthcare systems, public safety, and emergency operations. Infectious disease threats during such events are not limited to what spreads within stadiums.16
The broader challenge is that mass gatherings increase the likelihood that rare pathogens, travel-associated infections, or unfamiliar disease presentations will intersect with already strained care systems.
This is why preparedness for FIFA and similar events must include special pathogens awareness. Cities cannot rely only on traditional respiratory virus planning, food safety, or tropical medicine. They also need mechanisms to monitor global outbreak developments, translate those developments into updated screening and triage guidance, and coordinate rapidly across hospitals, public health agencies, emergency medical services, emergency management, and event organizers.
The Special Pathogens Biopreparedness Map can support this work in at least three ways.
First, it can support pre-event risk assessment. Host cities can use the map to identify which high-consequence pathogens are currently active globally and build those risks into planning assumptions, tabletop exercises, and clinician education, including just-in-time training.
Second, it can support situational awareness during the event. If outbreak conditions shift internationally while mass gatherings are underway, operational leaders need a mechanism to quickly reassess travel screening questions, personal protective equipment considerations, reporting thresholds, and communication needs.
Third, it can support post-event surveillance and clinical vigilance. Patients often present after travel or exposure, not necessarily during the event itself. A tool that links outbreak context to bedside practice can help reduce delayed recognition in emergency departments, urgent care settings, and outpatient clinics.
This approach is consistent with the broader literature on infectious disease planning for mass gatherings, which emphasizes coordinated surveillance, rapid risk assessment, and strong cross-sector communication.17 The challenge is not simply to collect information. It is to turn information into decisions.
A TOOL, NOT A SUBSTITUTE
It is important to be clear about what a map can and cannot do. A biopreparedness map does not replace formal surveillance systems, laboratory diagnostics, or public health investigation. It does not predict when the next imported case will arrive. And it does not, by itself, create readiness.
What it can do is reduce the distance between awareness and action. It can help clinicians ask better questions. It can help hospitals refine their screening thresholds and escalation pathways. It can help emergency managers incorporate outbreak intelligence into planning for healthcare delivery, transportation, and mass gatherings. And it can help reinforce the broader principle that preparedness must be dynamic, not static.
That principle is increasingly important. Biological threats are not occurring in isolation. They are unfolding alongside strained health systems, misinformation, workforce fatigue, climate-linked disruptions, and heightened public scrutiny. In this environment, preparedness tools need to be practical, accessible, and grounded in operational use.
LOOKING AHEAD
The future of special pathogens preparedness will depend on whether health systems can move beyond static binders and toward living systems of readiness. That means integrating outbreak intelligence into routine workflows, making it easy for frontline clinicians to access disease-specific guidance, and ensuring that emergency management and public health teams are working from the same operational picture.
The Special Pathogens Biopreparedness Map reflects that shift. Developed within a large municipal health system in the United States and rooted in the lessons of the 2014 Ebola response, it is part of a broader “all-infectious-diseases” approach to biological preparedness. It is intended not to alarm, but to support disciplined readiness.
That is the core message. Special pathogens may be rare, but the consequences of delayed recognition can be severe, not just for local communities but also for regional and national levels. In an interconnected world, real-time situational awareness is no longer an added benefit. It is a prerequisite for safe, timely, and coordinated action.




