BACKGROUND AND AIMS
Arterial hypertension and renal involvement are increasingly recognised but still underdiagnosed complications in children and adolescents with neurofibromatosis.1,2 Neurofibromatosis type 1 (NF1) is caused by pathogenic variants in the NF1 gene on chromosome 17q11.2, encoding neurofibromin, a negative regulator of the RAS/MAPK pathway.3,4 Loss of neurofibromin function promotes abnormal vascular proliferation, intimal hyperplasia, medial thinning, and elastic lamina disruption, predisposing to arterial stenosis, aneurysmal change, and renovascular disease.4,5 Hypertension in NF1 may be either essential or secondary, with renal artery stenosis, middle aortic syndrome, phaeochromocytoma/paraganglioma, and coarctation of the aorta among the most important described secondary causes.3,6,7 This study aimed to evaluate the incidence, aetiology, and severity of hypertension and renal manifestations in a single-centre paediatric neurofibromatosis cohort.
MATERIALS AND METHODS
A single-centre retrospective cohort study was conducted at Hospital Sant Joan de Déu, Barcelona, Spain, including 475 paediatric patients with neurofibromatosis followed between July 2015–July 2025. Most patients had NF1 (94.6%), with a smaller proportion with NF2-related schwannomatosis. Data on blood pressure measurements, ambulatory blood pressure monitoring (ABPM), renal function, and imaging findings were collected. Hypertension was defined and classified according to current paediatric guidelines. ABPM was performed in clinically indicated cases and was also used to detect masked hypertension and to characterise blood pressure patterns. Secondary causes of hypertension were systematically investigated, including renovascular imaging when clinically warranted.
RESULTS
Of the 475 patients evaluated, 7.78% showed renal involvement and 4.21% had arterial hypertension.8 Kidney function was generally preserved, although clinically relevant findings included haematuria, proteinuria, and occasional chronic kidney disease. Hypertension was detected at a median age of 12.5 years.8 Of hypertensive cases, 70% were identified by ABPM, underscoring the diagnostic value of out-of-office blood pressure assessment in this setting.8 The most frequent cause of hypertension was pharmacological, followed by primary (essential) hypertension and vascular causes.8 Four patients had renal artery stenosis, and two required vascular intervention.8 Generalised systolic-diastolic hypertension was the most common ABPM pattern.8 Target organ injury, including microalbuminuria and mild ventricular hypertrophy, was present in a subset of patients.8 Cardiovascular disease-related findings in this cohort are also consistent with the broader literature describing NF1 as a condition with substantial cardiovascular risk (Figure 1).9
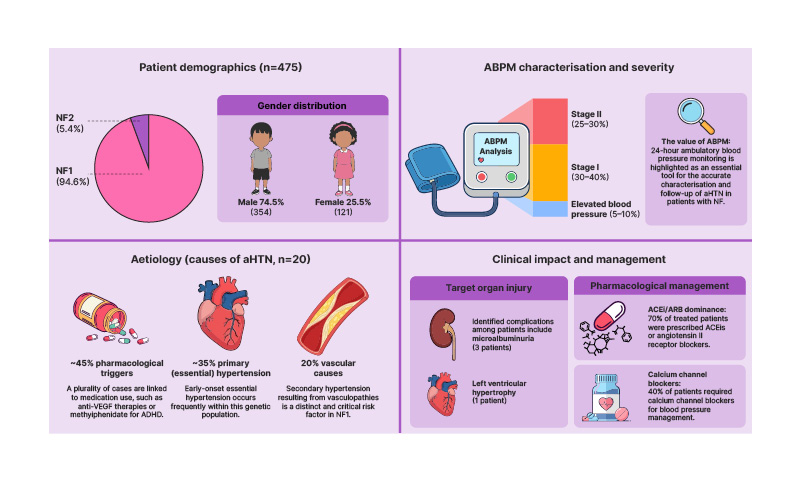
Figure 1: Arterial hypertension in paediatric patients with neurofibromatosis.
ABPM: ambulatory blood pressure monitoring; ACEi: angiotensin-converting enzyme inhibitor; aHTN: arterial hypertension; ARB: angiotensin II receptor blockers; NF: neurofibromatosis; VEGF: vascular endothelial growth factor.
CONCLUSION
Hypertension in NF1 should not be considered an incidental finding, but rather part of a broader vascular phenotype with potential consequences for long-term morbidity.1,6,10 These findings reinforce the need for systematic blood pressure surveillance in paediatric neurofibromatosis, ideally beginning in early childhood and continuing through adolescence.3,6 Any confirmed hypertension should prompt structured evaluation for secondary causes, including renovascular imaging when clinically indicated, particularly in children with severe, early-onset, or difficult-to-control hypertension.3,6,10 Additional contributors such as chronic pain, anxiety, stimulant drugs, and anti-vascular endothelial growth factor therapies may increase blood pressure burden and complicate clinical interpretation.2,3,7,11 Ambulatory blood pressure monitoring is particularly useful not only for diagnosis, but also for phenotyping hypertension severity, detecting masked hypertension, and guiding follow-up.8 A multidisciplinary approach, including paediatric nephrology, oncology, cardiology, neurology, and clinical genetics, is appropriate for early recognition of vascular complications, prevention of target organ damage, and individualised treatment.1,2,8 Early detection by regular blood pressure assessment and ABPM may improve long-term vascular and renal outcomes in this population.8






