BACKGROUND AND AIMS
Haemodialysis is associated with substantial psychological burden for both patients and their family caregivers. Preliminary findings of this study suggest that caregiver acceptance-focused coping may help buffer the spillover of anxiety within haemodialysis dyads.¹
Cumulative evidence shows the interdependence of emotional wellbeing in patient-caregiver dyads, in which psychological strain experienced by one member may negatively affect the other.² Such bidirectional processes may contribute to cycles of shared distress and maladaptive psychosocial adjustment to chronic illness.2 Acceptance-focused coping, characterised by the ability to experience difficult emotions and circumstances without excessive avoidance or psychological resistance,3 has previously been associated with greater psychological flexibility and improved psychosocial adjustment among family caregivers in kidney failure.⁴ Nevertheless, its role in haemodialysis dyadic adaptation has not been fully explored.
This study examined whether caregiver acceptance-focused coping moderated the relationship between patient anxiety and caregiver anxiety and burden, as well as its effects on patient quality of life.
MATERIALS AND METHODS
This was a cross-sectional study involving 68 haemodialysis patient–caregiver dyads, of which 44% were couples. Patients and caregivers completed a set of validated health-related self-report measures assessing anxiety symptoms using the Hospital Anxiety and Depression Scale-Anxiety (HADS-A) subscale and quality of life using the WHO Quality of Life-BREF (WHOQOL-BREF) questionnaire. Caregivers also completed the Zarit Burden Interview (caregiver burden) and the acceptance subscale of the Brief COPE. Statistical analyses were performed using the PROCESS macro (Model 58) in Statistical Package for the Social Sciences (SPSS; IBM Corporation, Armonk, New York, USA) to test a moderated parallel mediation model, with all predictors mean-centred before analysis.
RESULTS
Higher patient anxiety was directly associated with poorer patient quality of life (B=−1.124; p=0.023), while caregiver acceptance-focused coping moderated the relationship between patient anxiety and caregiver anxiety (B=0.378; p=0.019), suggesting a buffering effect within the dyad. This interaction indicated that caregivers with higher acceptance-focused coping scores appeared less susceptible to the emotional impact of patient anxiety. Indirect effects of patient anxiety on patient quality of life through caregiver anxiety or caregiver burden were not statistically significant. Figure 1 illustrates the moderated mediation model of the relationship between patient anxiety, caregiver anxiety and burden, and patient quality of life.
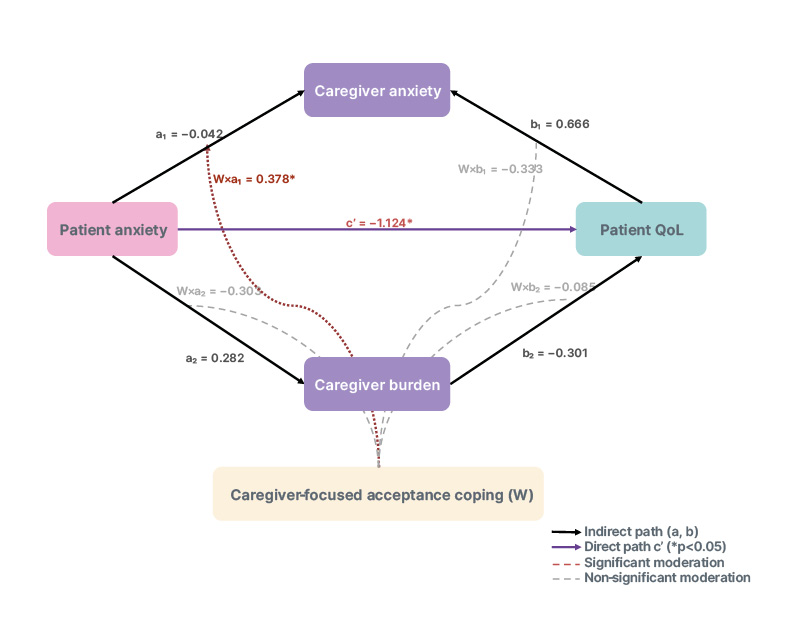
Figure 1: Moderated mediation model of the relationship between patient anxiety, caregiver anxiety and burden, and patient quality of life.
*p<0.05.
Note: unstandardised coefficients (B). All predictors mean-centred. p values: a₁: p=0.702; a₂: p=0.510; b₁: p=0.262; b₂: p=0.087; c′: p=0.023*; W×a₁: p=0.019*; W×a₂: p=0.625; W×b₁: p=0.578; W×b₂: p=0.606.
CONCLUSION
Findings suggest that acceptance-focused coping may operate primarily at the caregiver level by mitigating emotional strain associated with haemodialysis caregiving and buffering the interpersonal transmission of anxiety within patient-caregiver dyads. Acceptance-based interventions targeting both patients and caregivers, such as acceptance and commitment therapy, may therefore offer a promising avenue for reducing shared distress and supporting adaptive psychosocial functioning within haemodialysis dyads. Such dyadic approaches may be particularly relevant in haemodialysis settings, where caregiver burden and distress frequently remain underrecognised.5 Although large longitudinal studies are needed to clarify these bidirectional psychological pathways further, the present findings reinforce the clinical relevance of integrating family caregivers into psychosocial interventions and also support family-centred models in nephrology practice.






