This is a promotional article developed by GSK. Content was generated through interviews with experts. These experts were paid by GSK for their services. This article is intended for Healthcare Professionals only.
Interviewees: John Blakey1-3, Christian Domingo4,5
1. Curtin University, Perth, Australia
2. University of Western Australia, Perth, Australia
3. Sir Charles Gairdner Hospital, Nedlands, Australia
4. Pulmonary Service, Corporació Parc Tauli, Sabadell, Spain
5. Department of Medicine, Universitat Autònoma de Barcelona, Spain
Support: This is a promotional article developed by GSK. Content was generated through interviews with experts. These experts were paid by GSK for their services. This article is intended for Healthcare Professionals only.
Relvar Ellipta (fluticasone furoate, vilanterol) is indicated for the regular treatment of asthma in adults and adolescents aged 12 years and older where use of a combination medicinal product (long-acting β2-agonist and inhaled corticosteroid) is appropriate:
- patients not adequately controlled with inhaled corticosteroid and ‘as needed’ inhaled short-acting β2-agonists
- patients already adequately controlled on both inhaled corticosteroid and long-acting β2-agonist
UK Prescribing Information can be found here.
Please refer to your local prescribing information for further information.
Adverse event reporting information can be found at the end of the article.
Disclosure: Over the last three years, either Blakey or his institution has received income from Asthma Australia, AstraZeneca, Boehringer Ingelheim, Chiesi, GSK, and Sanofi. Grant support has also come from FHRI, MRFF, IPCRG, and Avant.
Domingo received an honorarium from GSK for this presentation and reports having previously received fees from GSK, Novartis, Sanofi, Teva, Esteve, AstraZeneca, Chiesi, Menarini, Stallergenes, ALK-Abelló, Allergy Therapeutics, and Inmunotek.
Acknowledgments: Medical writing assistance was provided by Yolande Chalmers, EMJ, London, UK.
Disclaimer: This article is based on a promotional interview organised by GSK for healthcare professionals in countries where Relvar Ellipta (fluticasone furoate, vilanterol) is indicated for the regular treatment of asthma in adults and adolescents aged 12 years and older where use of a combination medicinal product (long-acting β2-agonist and inhaled corticosteroid) is appropriate: patients not adequately controlled with inhaled corticosteroid and ‘as needed’ inhaled short-acting β2-agonists, or patients already adequately controlled on both inhaled corticosteroid and long-acting β2-agonist.
Please refer to your local prescribing information for further information.
Keywords: Asthma, beclomethasone dipropionate (BDP), budesonide (BUD), ease-of-use, exacerbation reductions, exacerbation risk, fluticasone furoate (FF), formoterol (Form), inhaled corticosteroid/long-acting β2-agonist (ICS/LABA), quality of life, vilanterol (VI).
Citation: EMJ Respir. 2026;14[Suppl 1]:2-8. https://doi.org/10.33590/emjrespir/267P74V5
Interview Summary
Asthma is a prevalent respiratory condition that affects people of all ages, encompassing a range of subtypes. Exacerbations are common to those living with asthma, marked by a deterioration in symptoms and increased inflammation, leading to illness and the need to seek medical assistance. Consequently, a key pillar of asthma treatment is minimising exacerbation risk. In this interview, two leading experts and authors of the studies discussed the latest real-world evidence (RWE) on inhaled corticosteroid/long-acting β2-agonists (ICS/LABAs) for newly treated patients, exploring treatment persistence and exacerbation reduction. The discussion focuses on how evidence from the new RWE studies can inform preference towards a treatment choice for the appropriate management of asthma.
WHY DO WE NEED RWE IN ADDITION TO RCTs?
Asthma exacerbations have a significant impact on patients’ lives. Characterised by a deterioration in symptoms and increased inflammation, exacerbations often leave patients in need of medical assistance.1,2
John Blakey, Curtin University, University of Western Australia, Perth; and Sir Charles Gairdner Hospital, Nedlands, Australia, described that in his clinic, “one of the key things that patients [with asthma] fear is exacerbations. They do not want that feeling of being terribly breathless. They don’t want to have to turn up to the emergency department or miss work. If there’s one thing they can avoid, it’s exacerbations.” Asthma also negatively affects health-related quality of life and the ability to perform daily activities.1,2
The Global Initiative for Asthma (GINA) recommends two treatment tracks with ICS/LABAs for asthma guidelines in Steps 3 and 4.2 Track 1, the preferred option, includes low-dose (Step 3)/medium-dose (Step 4) ICS/formoterol (Form) maintenance and reliever therapy.2 Alternatively, Track 2 involves maintenance low-dose (Step 3) and medium-dose (Step 4) ICS, plus non-Form LABAs in patients with moderate-to-severe asthma, with as-needed short-acting β2-agonist (SABA).2 fluticasone furoate (FF), GINA classes FF 100 µg total daily as a low-medium dose, and FF 200 µg total daily as a medium-high dose.2
For beclomethasone (extrafine), GINA classes 100–200 µg total daily as low dose, >200–400 µg total daily as medium dose, and >400 µg total daily as high dose.2 For budesonide, 200–400 µg total daily is classed as low dose, >400–800 µg total daily is medium dose, and >800 µg total daily is high dose.2
Blakey highlighted that GINA considers data from randomised controlled trials (RCTs) more strongly than RWE when generating guidelines. This means that they may not accurately depict the complexity of treating patients in the real world, or accurately reflect clinical decision-making in practice. For example, he explained that whilst in RCTs adherence levels are high, in real-world patients, adherence is much lower.3,4 He added that RCTs often have restrictive entry criteria, which exclude groups of real-world patients who are not eligible. For example, those who are older, pregnant, or may smoke.
Over the past decade, FF/vilanterol (VI) has been compared to several other ICS/LABAs in a range of RCTs and, subsequently, real-world observational studies.5-12 Whilst RCTs are the gold standard for regulatory purposes,13 as Blakey put it, “RCTs ask ‘does this treatment work under ideal conditions?’ Whereas real-world studies ask, ‘does this treatment work [for the types of patients I treat]?’” Real-world studies provide a clearer view of treatment effectiveness in practice, reflecting both the diversity of patient populations and variations in adherence.14,15
With advances in big data, including large-scale electronic health records, insurance claims, and genomic datasets, regulatory bodies in the USA and Europe have formally recognised the role of real-world data to generate robust RWE, complementary to RCTs in regulatory decision-making.16,17 Nevertheless, RWE is not without its limitations, including issues related to completeness and data gaps.13
Whilst direct comparisons in controlled trials of ICS/LABAs with similar doses and regimens have shown comparable efficacy, RWE are needed to determine effectiveness in practice.15,18
EFFECTIVENESS OF ICS/LABAs IN NEWLY-TREATED PATIENTS, IN THE REAL WORLD
Two retrospective real-world effectiveness studies were carried out in a large general practice cohort in the UK. Study 1 investigated the rate of exacerbations in new users of FF/VI (n=3,773) versus new users of beclomethasone dipropionate (BDP)/Form (n=46,809), with a subgroup analysis of patients who stepped up from ICS plus SABA (FF/VI: n=1,599; BDP/Form: n=23,197).19,20 Study 2 similarly investigated the rate of exacerbation in new users of FF/VI (n=3,774) but compared with new users of budesonide (BUD)/Form (n=14,464), again with a subgroup analysis of patients who stepped up from ICS plus SABA (FF/VI: n=1,474; BUD/Form: n=3,798).21,22
In accordance with the approved indication for FF/VI (in the EU and countries with an EU-like indication), this article focuses on the findings from the specific patient population who stepped up from ICS plus SABA at baseline.
Patients who initiated treatment with BDP/Form, BUD/Form, or FF/VI between 1st December 2015–28th February 2019 (index period) were selected from anonymised Clinical Practice Research Datalink (CPRD) data and Hospital Episode Statistics (HES) data. Those observed were ≥18 years of age with an asthma diagnosis at index and had been prescribed either FF/VI, BUD/Form, or BDP/Form. Patients had at least one prescription of a SABA inhaler in the 6 months prior to the index date. Patients with chronic obstructive pulmonary disease (COPD) and those with ≥1 fixed dose ICS/LABAs, single inhaler triple, or biologic therapy were excluded.19,21
The primary study outcome was the rate of overall (moderate-severe) asthma exacerbations (per patient per year), with secondary outcomes including time to first asthma exacerbation and exacerbation rates, as stratified by index dose, as well as medication persistence and oral corticosteroid (OCS) use.19,21 Subpopulation rate analyses were calculated as per patient per day (PPPD) and not per patient per year.20,22
Statistical analysis of the primary endpoint consisted of three estimands: while-on index treatment analyses (primary estimand) considered measurements until the time of an intercurrent event (treatment switching, discontinuation, loss to follow-up, death, and rescue medication use); on index treatment analyses (supplementary estimand one) considered measurements regardless of whether an intercurrent event occurred; and continued index treatment for 12 months without interruption analyses (supplementary estimand two; ‘principal stratum’) only included patients not experiencing an intercurrent event.19-22
One limitation of the studies was the use of retrospective database methodology, which may have introduced selection bias and potentially affected the generalisability of the results. In addition, the medications may not have been consumed as prescribed, patients with COPD could be misidentified as patients with asthma, and the databases used may have inconsistently coded or underreported asthma exacerbations. Finally, although efforts were undertaken to adjust for baseline differences between the study groups via inverse probability of treatment weighting, residual confounding from unmeasured variables remains a potential study limitation, as with any observational study.19,21
In Study 1, the rate of exacerbations in the subpopulation of patients who stepped up from ICS plus SABA (primary estimand) was similar for FF/VI and BDP/Form (0.00036 versus 0.00039 PPPD, respectively; hazard ratio [HR]: 0.92; p=0.35). However, patients who stepped up from ICS plus SABA and continued treatment uninterrupted for 12 months (supplementary estimand two) with FF/VI (n=257) had a 44% lower exacerbation rate versus BDP/Form (n=2,794; 0.0002 versus 0.0003 PPPD, respectively; HR: 0.559; p=0.031; Figure 1).20
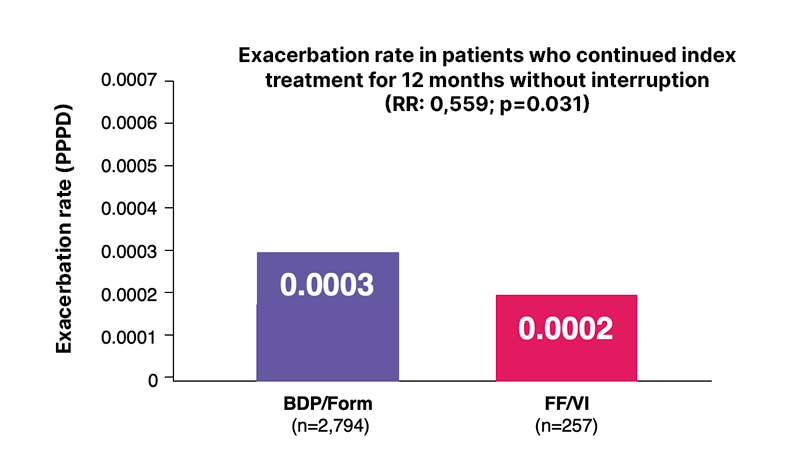
Figure 1: Exacerbation rate (PPPD) in Study 1 (subpopulation supplementary estimand two).
Adapted from Woodcock et al.20
BDP: beclomethasone dipropionate; FF: fluticasone furoate; Form: formoterol; PPPD: per patient per day;
RR: rate ratio; VI: vilanterol.
Moreover, Study 2 showed that the rate of exacerbations in the subpopulation of patients stepping up from ICS plus SABA (primary estimand) were similar between FF/VI and BUD/Form (0.0003 vs 0.0005 PPPD); with a trend towards FF/VI, although this did not reach statistical significance (HR=0.75; p=0.10). In those that stepped up from ICS plus SABA for 12 months of uninterrupted treatment (supplementary estimand two), FF/VI (n=245) had a 70% lower exacerbation rate versus BUD/Form (n=300; 0.0002 versus 0.0006 PPPD, respectively; HR: 0.3; p=0.0013; Figure 2).22
The results in the step-up population were consistent with the overall study population.19-22
Regarding the subpopulation outcomes from the RWE, Blakey explained: “In this real-world study, patients adhering to FF/VI over a period of 12 months [showed a lower rate of exacerbations] compared to those on combination BUD/BDP with formoterol […] this gives [clinicians] information to incorporate into treatment decisions, monitoring our patients, when making prescription choices for our patients.”
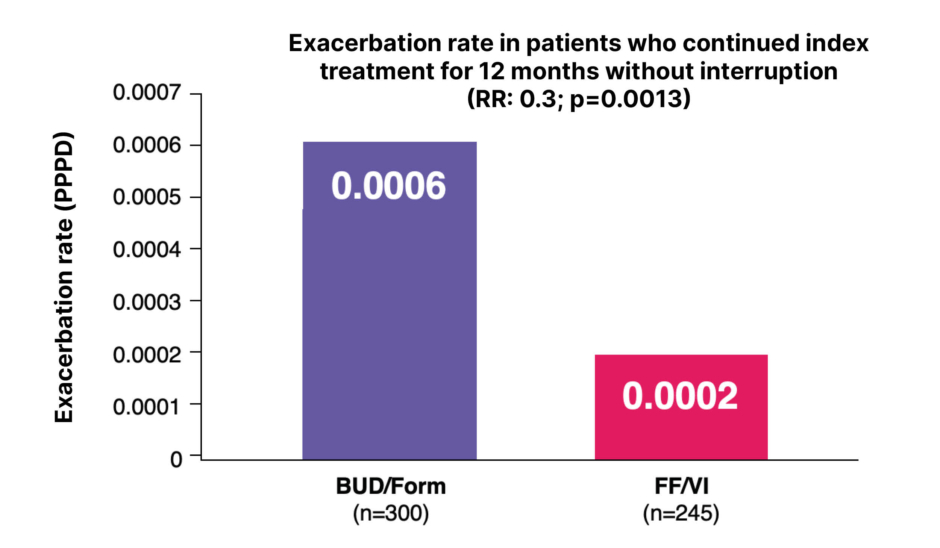
Figure 2: Exacerbation rate (PPPD) in Study 2 (subpopulation supplementary estimand two).
Adapted from Woodcock et al.22
BUD: budesonide; FF: fluticasone furoate; Form: formoterol; PPPD: per patient per day; RR: rate ratio; VI: vilanterol.
He maintained that whilst achieving a reduction in exacerbations is key to informing management decisions, it is important to consider other endpoints to aid patients in living well with asthma.
HELPING PATIENTSLIVE WELL WITH ASTHMA
Christian Domingo, Pulmonary Service, Corporació Parc Tauli, Sabadell; and Department of Medicine, Universitat Autònoma de Barcelona, Spain, acknowledged the importance of exacerbation reduction, yet emphasised that exacerbation reduction is not the sole factor clinicians should consider when prescribing a treatment for a patient with asthma.
Domingo put it succinctly: “It is, of course, relevant to decide on which drug to treat the patient with, but if the patient doesn’t follow the treatment, or does not administer it correctly, then the drug will not even begin to take effect.”
Treatment Persistence
Regarding treatment persistence in the new RWE, results showed FF/VI had greater treatment persistence than other ICS/LABAs (BUD/Form and BDP/Form) among patients stepping up from ICS plus SABA.20,22 FF/VI demonstrated significantly higher treatment persistence than BDP/Form or BUD/Form at 12 months.20,22
At 12 months, patients stepping up from ICS plus SABA were 24% less likely to discontinue FF/VI (N=1,283) versus BDP/Form (N=19,323) following step up from ICS plus SABA (HR: 0.76; p<0.0001).20 Patients remaining on treatment at 12 months: 15.4% (n=197) for FF/VI versus 10.3% (n=1,990) for BDP/Form.23 HR for treatment persistence is 0.76; p<0.0001 (secondary endpoint).20
Patients were also 31% less likely to discontinue FF/VI (N=1,282) versus BUD/Form (N=3,328) following step up from ICS plus SABA (HR: 0.69; p<0.0001).22 Patients remaining on treatment at 12 months: 14.4% (n=185) for FF/VI versus 6.7% (n=222) for BUD/Form.23 HR for treatment persistence is 0.69; p<0.0001 (secondary endpoint).22
The persistence was low for all treatments.
FF/VI and OCS Exposure
Another key consideration, Domingo noted, is OCS exposure. In the two recently published real-world studies, in patients stepping up to FF/VI from ICS plus SABA, there was equivalent cumulative OCS prescription versus BDP/Form (mean number of OCS prescriptions per patient per year: 0.37 for FF/VI [n=1,483] versus 0.34 for BDP/Form [n=21,643]; rate ratio for cumulative OCS dosage: 0.69; significance threshold not met [p=0.11]).20
In patients stepping up from ICS plus SABA, there was a 49% lower cumulative OCS dosage for FF/VI versus BUD/Form (mean number of OCS prescriptions per patient per year: 0.3 for FF/VI [n=1,368] versus 0.49 for BUD/Form [n=3,497]; rate ratio for cumulative OCS dosage: 0.51; p=0.043).22
Overall, in the studies presented above, it was observed that patients on FF/VI had improved persistence versus BDP/Form and BUD/Form and reduced reliance on OCS use versus BUD/Form.20,22,23 Real-world data on exacerbation reduction support FF/VI as an appropriate treatment choice for the management of asthma.20,22
These RWE did not collect safety data; however, data from large asthma and COPD clinical trials were used to determine the frequency of adverse reactions associated with FF/VI.24 The most commonly reported (≥1/10) adverse reactions were headache and nasopharyngitis.24 Pneumonia is one of the commonly reported (≥1/100) adverse reactions.24 Cardiac disorders are either uncommon (≥1/1,000–<1/100) or rare (≥1/10,000–<1/1,000).24
CONCLUSION
The new RWE discussed by Blakey and Domingo has shown that, while overall exacerbation rates between the three ICS/LABAs were similar in the primary and secondary estimands, when stepping up from ICS plus SABA and continuing treatment uninterrupted for 12 months (secondary estimand), FF/VI significantly reduced exacerbations compared to BDP/Form and BUD/Form.20,22 The same studies also show that FF/VI has greater treatment persistence versus BDP/Form and BUD/Form.20,22
Overall, the studies contribute valuable real-world insight to existing evidence, highlighting FF/VI as an ICS/LABAs combination that may improve some patient outcomes in clinical practice when compared to other ICS/LABAs therapies.
Domingo and Blakey both agreed that this recent RWE builds upon and strengthens the existing evidence base, offering clinical insights beyond the findings of RCTs. These data provide a holistic understanding of ICS/LABAs treatment effectiveness and adherence. Together, this evidence aids clinicians in making informed prescribing decisions for their patients.
| Adverse events should be reported. Reporting forms and information can be found at https://yellowcard.mhra.gov.uk/ or search for MHRA Yellowcard in the Google Play or Apple App store. Adverse events should also be reported to GSK on 0800 221 441 or [email protected]. |
Job Code: PM-GBL-FFV-ADVR-250006
DOP: June 2026





