BACKGROUND AND AIMS
Primary hyperparathyroidism (PHPT) is one of the most common endocrine disorders, characterised by excessive parathyroid hormone secretion and resulting in accelerated bone resorption, with osteoporosis affecting up to 62.5% of patients in the Russian population.1,2 Parathyroidectomy (PTE) as the only curative treatment2 is well documented to significantly improve bone mineral density (BMD) following surgery. However, bisphosphonates (BPh) remain an option for correcting hypercalcaemia and improving bone status in patients who cannot undergo surgery.3 Given the prolonged skeletal half-life of BPh (up to 10 years), a key question arises: does prior BPh exposure impair the natural bone recovery that follows successful PTE? This question remains unresolved, and no consensus exists regarding continuation or initiation of antiresorptive therapy in the peri-operative setting.2,4,5
MATERIALS AND METHODS
This single-centre, retrospective, observational study was conducted at the Department of Parathyroid Pathology and Mineral Metabolism Disorders, I.I. Dedov Endocrinology Research Centre, Moscow, Russia. Fifty patients (48 women and two men) with verified PHPT who underwent successful PTE between October 2016–February 2024 were enrolled. Participants were divided into two groups based on pre-operative treatment: Group 1 (n=25) had received BPh prior to surgery (median duration: 15 months), and Group 2 (n=25) had received no antiresorptive therapy. Groups were matched for sex, age, and baseline BMD values at three skeletal sites. Dual-energy X-ray absorptiometry (DXA) scans were assessed at the lumbar spine (LS), total hip (TH), femoral neck (FN), and distal radius. 3D-DXA analysis of the proximal femur was performed using 3D-Shaper® (3D-Shaper Medical, S.L., Barcelona, Spain) Medical software (v2.12.1), providing cortical surface BMD, cortical volumetric BMD (vBMD), cortical thickness, and trabecular vBMD. Statistical analysis included the Wilcoxon signed-rank test for within-group comparisons and the Mann–Whitney U-test for between-group comparisons, with Bonferroni correction applied for multiple testing.
RESULTS
At baseline, the two groups were comparable across all key biochemical and DXA parameters, with the exception of β-crosslaps, which was significantly higher in Group 2 (median: 1.315; interquartile range [IQR]: 1.010–1.720 ng/mL versus median: 0.531; IQR: 0.305–0.976 ng/mL; p=0.0003), reflecting greater pre-operative bone turnover. Pre-operative 3D-DXA parameters did not differ between groups. Between-group comparison of absolute BMD gains at 1-year post-PTE revealed no statistically significant differences at any DXA site. However, 3D-DXA final absolute values showed a trend toward higher cortical thickness at the TH (median: 1.90; IQR: 1.80–1.96 mm versus median: 1.78; IQR: 1.71–1.84 mm; p=0.006) and FN (median: 1.63; IQR: 1.52–1.70 mm versus median: 1.50; IQR: 1.40–1.62 mm; p=0.013) in Group 2, approaching but not reaching the Bonferroni-corrected threshold. Within-group analysis revealed a broader and more consistent pattern of bone recovery in Group 2. Statistically significant improvements were observed at the LS, TH, and FN by DXA, and at three 3D-DXA parameters: trabecular vBMD at TH and FN, and cortical surface BMD at TH. In contrast, Group 1 demonstrated significant improvement only at the LS by DXA and in trabecular vBMD at TH by 3D-DXA, with no significant change in cortical parameters (Figure 1)
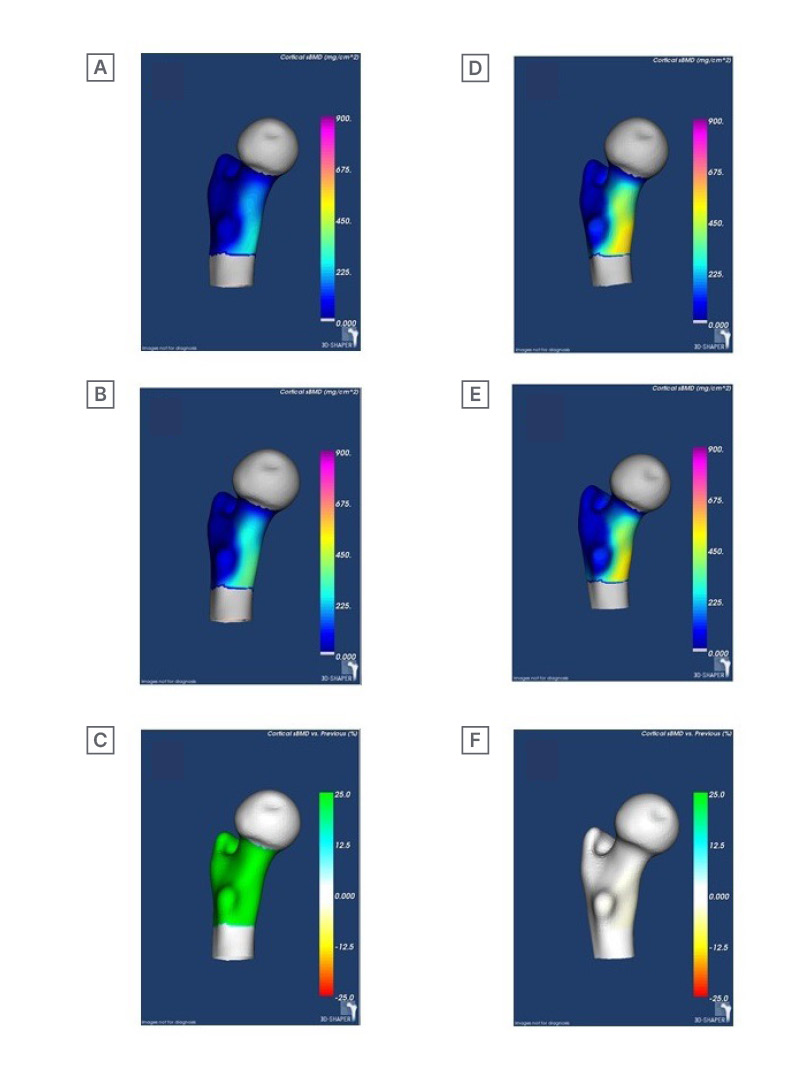
Figure 1: 3D-shaper visualisation of cortical surface BMD over time.
A–C) Patient from Group 1; and D–F) patient from Group 2. A) and D) cortical surface BMD of the dorsal proximal femur before PTE (mg/cm²); B) and E) cortical surface BMD of the dorsal proximal femur after PTE (mg/cm²); and C) and F) change in cortical surface BMD of the dorsal proximal femur before and after PTE; the change in cortical surface BMD is expressed as percentage gain after PTE relative to pre-PTE cortical surface BMD (%).
BMD: bone mineral density; PTE: parathyroidectomy.
CONCLUSION
This study provides novel evidence that pre-operative BPh therapy may attenuate post-PTE bone recovery, particularly with respect to cortical bone compartments as assessed by 3D-DXA. While standard DXA showed comparable gains between groups, 3D-DXA revealed a trend toward greater cortical restoration in patients without prior BPh exposure. BPh can suppress the osteoclast-mediated remodelling that is physiologically essential after PTE for replacing defective bone with structurally sound tissue. Thus, prior BPh use may limit the magnitude of this anabolic response. These findings highlight the clinical importance of 3D-DXA as a sensitive tool for monitoring bone microarchitecture in PHPT and underscore the need for prospective studies with larger cohorts and longer follow-up to clarify the optimal management of antiresorptive therapy in this setting.






