BACKGROUND AND AIMS
The orthogeriatric concept was introduced in the 1960s to address the impact of hip fractures on health systems.¹ Over the past 15 years, orthogeriatrics has evolved into a comprehensive model of care that includes multidisciplinary management of patients with fractures, involving geriatricians, pre-operative preparation, pain management, and continuity of care after discharge.² In parallel, effective risk communication with older adults has become increasingly important, as it is closely linked to decision-making processes and the development of health-related communication strategies throughout the ageing process.3 The objective of this study was to assess risk perception, chronic pain patterns, and bone health-related behaviours among elderly patients with chronic conditions in primary healthcare settings, and to identify key barriers and facilitators for orthogeriatric success.4 Particular emphasis was placed on the role of risk communication and a patient–family–healthcare practitioner-centred approach in optimising osteoporosis prevention, fracture reduction, and engagement with health services.
MATERIALS AND METHODS
This research integrates findings from several cross-sectional and observational studies conducted in Albania between 2017–2024, including primary healthcare centres and a regional hospital. Data were collected from healthcare professionals and elderly patients with chronic conditions (mean age ≥65 years) using structured questionnaires, focus group discussions, and retrospective clinical record reviews. Variables included sociodemographic characteristics, professional backgrounds of healthcare staff, and types of chronic non-oncological pain, osteoporosis risk factors, fracture patterns, patient education strategies, and perceptions of risk communication during health emergencies. Screening tools, such as the International Osteoporosis Foundation (IOF) One-Minute Osteoporosis Risk Test, were applied in community settings. Statistical analyses were performed using SPSS (IBM, Armonk, New York, USA), with significance set at p<0.05.
RESULTS
Healthcare providers were predominantly female (86.7%), with a mean age of approximately 30 years, and over half (57.5%) had ≤5 years of professional experience. Most were based in urban centres (85%). Chronic non-oncological pain was highly prevalent, with chronic back pain (70.8%) and joint pain (61.7%) being the most frequently reported conditions. Among elderly patients, frequent falls (22%), low-impact fractures (15%), thyroid disorders (50%), diabetes (40%), low BMI, smoking, and family history were common osteoporosis-related risk factors. Fractures were more frequent in men, particularly hip fractures in those aged ≥60 years, and were predominantly caused by falls and visual impairment. Patient education relied mainly on individual counselling (68.3%) and family involvement (50.8%), while formal educational seminars were limited (9.2%). Identified barriers included low trust in health authorities, fragmented risk communication, insufficient clinical documentation, and limited access to specialised resources (51.7%). Facilitators included physiotherapy involvement (48.3%) and cost-effective community screening tools (Figure 1).
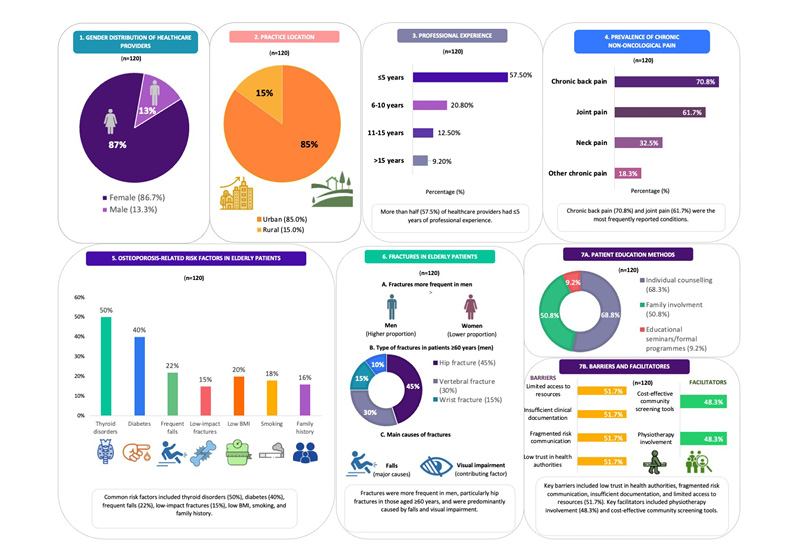
Figure 1: Key results of the study.
CONCLUSION
Optimising bone health behaviours in older adults requires strengthened risk communication, interdisciplinary orthogeriatric collaboration, and active engagement of patients and families. Addressing communication gaps, improving professional training, enhancing documentation quality, and expanding access to preventive screening and rehabilitation services are essential to reducing fractures and improving outcomes in ageing populations (Figure 2).
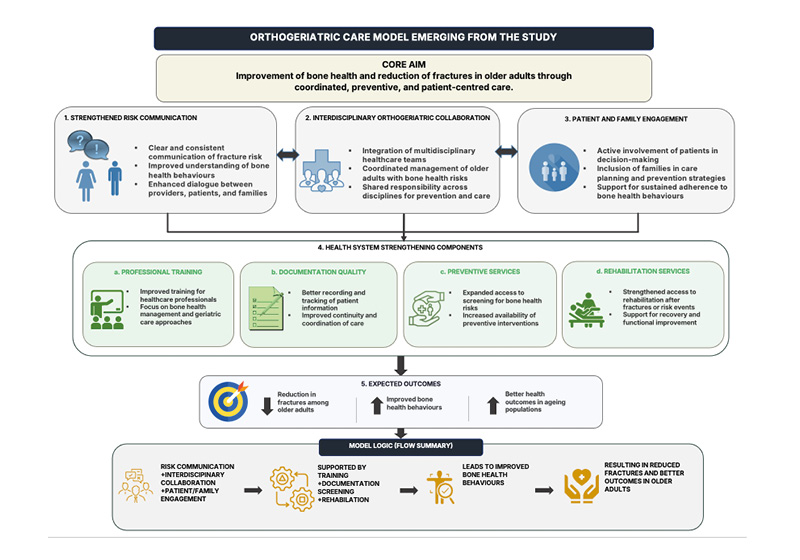
Figure 2: Orthogeriatric care model.
Orthogeriatric care model: an integrated model based on evidence from Albania (2017–2024), AI-generated using data derived from the conclusions of this study.






