BACKGROUND AND AIMS
Structural damage, particularly new bone formation (NBF) and progression thereof in the spine, is a well-recognised feature of axial spondyloarthritis (axSpA). However, detecting structural damage progression in the spine has been challenging due to the low sensitivity to change of radiography, which is the conventionally used imaging technique.1
In recent years, newer imaging modalities, including low-dose CT (ldCT) and MRI-based synthetic CT (sCT), have been investigated for their ability to detect structural spinal damage.2,3 sCT is a quantitative 3D MRI technique based on a multiple gradient-echo sequence and a deep-learning processing pipeline that can generate CT-like images without ionising radiation.
To the authors’ knowledge, no studies have evaluated the ability of ldCT to detect NBF-progression in the entire spine over time intervals shorter than 2 years, and no longitudinal studies of sCT of the spine have been conducted.
The aim of this study was to descriptively evaluate the capability of ldCT and sCT to detect the presence of NBF at baseline, and particularly the progression of NBF over 1 year in the spines of patients with axSpA.
MATERIALS AND METHODS
Participants underwent whole-spine ldCT and MRI at baseline and after 1 year. sCT images were reconstructed using BoneMRI v1.8 (MRIGuidance, Utrecht, the Netherlands). One reader assessed NBF (marginal and non-marginal syndesmophytes, osteophytes) at all vertebral levels, blinded to other imaging and clinical data but unblinded to chronology. Lesions were scored as 1 if present and non-bridging and 3 if bridging between vertebral units. Non-bridging lesions judged larger at one timepoint were registered. Progression was defined as new or enlarging lesions, regression as the reverse. Sensitivity, specificity, and accuracy of sCT were calculated using ldCT as the reference standard. Inter-modality agreement was assessed with intraclass correlation coefficients.
RESULTS
Twenty-five patients with axSpA were included (16 males; mean age: 52.7 years). At baseline, a mean of 21.7 marginal syndesmophytes per patient was scored across the entire spine on ldCT, along with 6.2 non-marginal syndesmophytes and 10.3 osteophytes. At Year 1, mean ldCT scores per patient increased to 22.7 marginal syndesmophytes, 6.5 non-marginal syndesmophytes, and 11 osteophytes, corresponding to mean increases of 1.0,
0.3, and 0.7, respectively.
On sCT, baseline whole-spine scores per patient were 29.6 for marginal syndesmophytes, 4.8 for non-marginal syndesmophytes, and 5.7 for osteophytes. At Year 1, these increased to 32.0, 5.5, and 6.5, corresponding to mean per-patient increases of 2.4 marginal syndesmophytes, 0.7 non-marginal syndesmophytes, and 0.8 osteophytes (Figure 1). Progression of marginal syndesmophytes was observed in seven patients on ldCT and 21 on sCT; regression in two and 13, respectively. Similar ldCT/sCT differences were seen for the other NBF-types, with most changes in the thoracic spine.
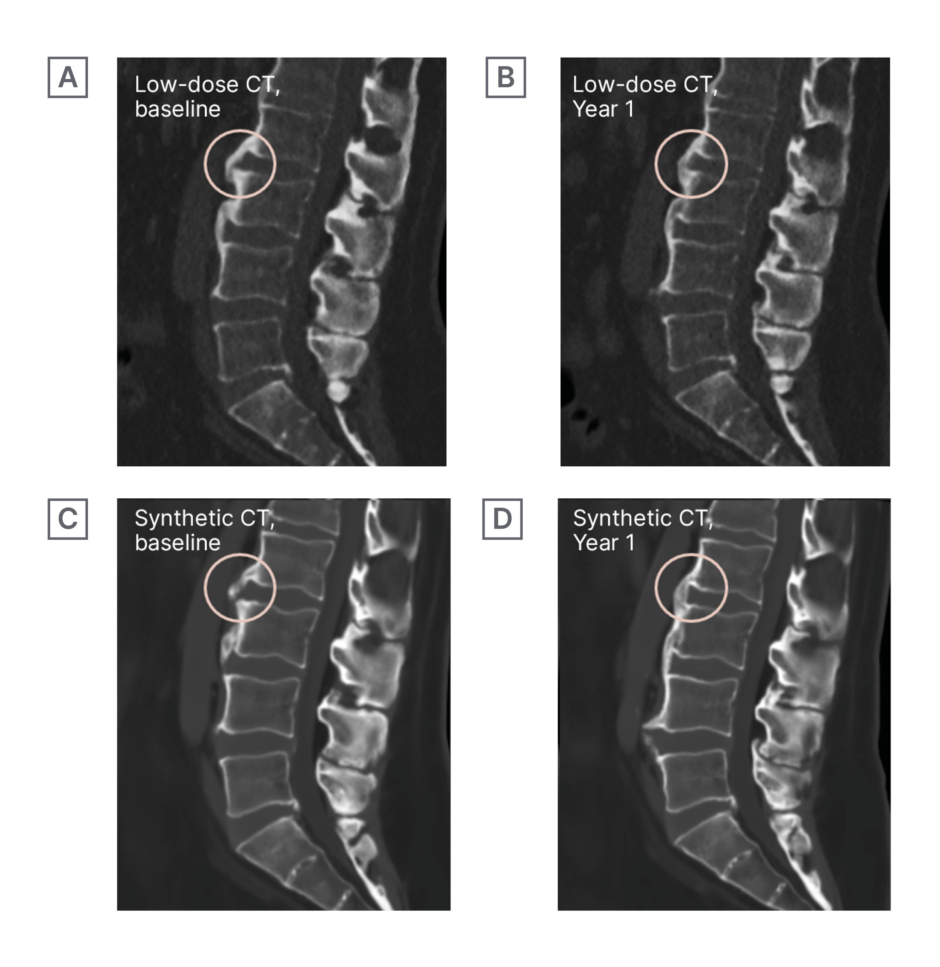
Figure 1: Low-dose CT and MRI-based synthetic CT images of the lumbar spine from the same patient at baseline (A, C) and at 1-year follow-up (B, D).
Circled regions demonstrate progression of new bone formation on both imaging modalities, with a non-bridging lesion at baseline (A,C) evolving into a bridging lesion at follow-up (B, D).
Using ldCT as the reference standard, the sensitivity of sCT for detecting marginal syndesmophytes was 0.81/0.81 (baseline/Year 1); for non-marginal syndesmophytes, 0.54/0.54; and for osteophytes, 0.41/0.42. Specificity and accuracy were ≥0.91.
Intraclass correlation coefficients between ldCT and sCT were 0.90/0.87 (baseline/ Year 1) for marginal syndesmophytes, 0.79/0.81 for non-marginal syndesmophytes, and 0.50/0.58 for osteophytes.
CONCLUSION
One-year progression of spinal NBF in patients with axSpA was observed on both sCT and ldCT. More patients showed progression on sCT than on ldCT; however, the overall magnitude of change for all lesions was comparable between modalities. Given the radiation-free nature of sCT and the excellent specificity and accuracy, this method, together with ldCT, holds promise for longitudinal assessment of spinal structural damage in axSpA.






