BACKGROUND
Appropriate use of antibiotics is critical to combat antimicrobial resistance (AMR) and optimise patient outcomes. At the East Kent University Hospitals NHS Foundation Trust (EKHUFT), broad-spectrum antibiotics (BSA) consumption has increased threefold over the past decade in the Watch and Reserve category (Define©).1 The UK National Action Plan sets clear targets for reducing antimicrobial use by 2029.2 Evidence shows that antimicrobial stewardship (AMS) interventions designed using behaviour-change principles (including prescriber commitment, audit and feedback, decision support, and peer comparison) can significantly reduce inappropriate antibiotic use, improving patient outcomes and supporting AMR reduction.3
AIM
To define a new AMS strategy that identifies AMS activities incorporating behaviour-change principles and assess its impact on broad-spectrum antibiotic prescribing across the Trust.4
METHODS
A series of AMS-focused activities was developed through regular multidisciplinary (MDT) meetings involving pharmacists, nurses, microbiologists, and clinicians.A prospective analysis was carried out over 2 consecutive years across adult inpatients in the authors’ 1,050-bed Trust. A series of AMS-focused activities was developed prospectively through regular MDT meetings involving pharmacists, nurses, microbiologists, and clinicians.
The main key drivers were grouped in five themes: 1) guideline and policy governance; 2) antimicrobial prescribing quality; 3) diagnostics; 4) in-patient and outcome-focused audits; 5) education and culture.
Prescribing behaviours were assessed in different stages, depending on audits conducted at admission, during inpatient stay, and at discharge.
Key activities explored included: guideline compliance; ward risk-based C. difficile key performing indicator-audits; documentation quality; timeliness of antimicrobial review; indication of antimicrobials with guidelines; guideline development and updates; optimisation of prescribing decisions; use of diagnostics prior to antibiotic initiation in acute medical units; surgical prophylaxis practice; AMS education delivery; and AMS policy revision.
RESULTS
Over 10 different activities were conducted involving different specialties. There was a reduction of BSA consumption over a 2-year period, plateauing the graph for consumption (stabilising a previously rising trend) with a 2.7% decrease in BSA and a 5.3% decrease in the Watch and Reserve category usage compared to the 2023 peak (Figure 1).
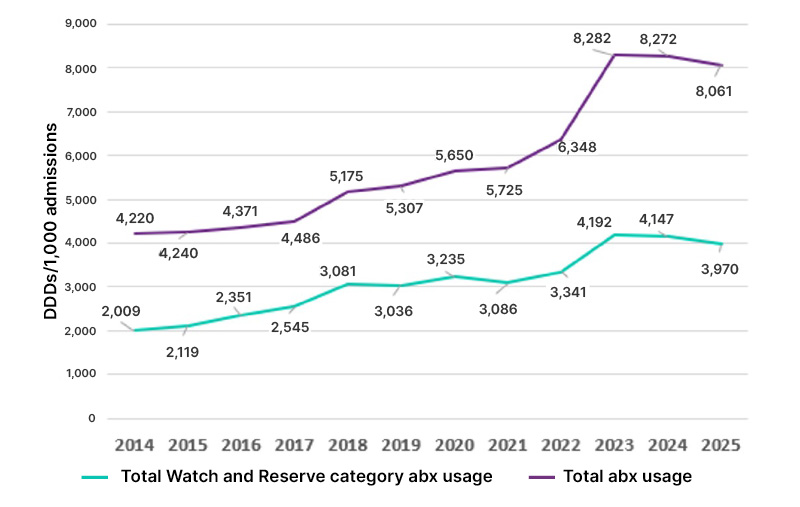
Figure 1: Total antibiotic versus ‘Watch and Reserve’ antibiotic consumption at EKHUFT in DDD/1,000 admissions (2014–2024; including FP10 data).
abx: antibiotics; DDD: daily defined dose; EKHUFT: East Kent University Hospitals NHS Foundation Trust.
There was greater awareness of AMS through MDT participation in audits and active communications.
Engagement with AMS education was mixed; training required targeted delivery and was not implemented as widely as initially planned. The AMS team took feedback from clinicians who wanted to see the impact on patients rather than daily defined dose data alone, so the authors used C.difficile infections as a measure to raise awareness amongst them.
CONCLUSION
A structured AMS strategy incorporating behavioural-change interventions can reduce BSA use and improve prescribing quality. Continued monitoring and reinforcement are required to sustain behaviour change and ensure long-term impact. Pharmacy-led AMS teams play a crucial role in driving improvements when a clear strategy is implemented.




