Abstract
Mycobacterium genavense is a rare, slow-growing non-tuberculous mycobacterium that primarily affects immunocompromised individuals, particularly those with advanced HIV. Due to its fastidious growth requirements and prolonged incubation period, conventional culture techniques frequently fail to detect the organism, delaying diagnosis and treatment. Molecular diagnostics such as PCR and 16S ribosomal RNA sequencing may improve detection, but their use is not yet standardised.
The authors present three cases of M. genavense infection in patients with advanced HIV/AIDS. All patients exhibited profound immunosuppression, with cluster of differentiation 4 (CD4) counts ranging from 1–82 cells/µL, and presented with prolonged fevers, pancytopenia, and multi-system involvement including lymphadenopathy, hepatosplenomegaly, and/or neurological symptoms. Conventional cultures remained negative in all cases despite extended incubation, with culture-negative specimens requiring diagnosis through terminal acid-fast bacilli smears and molecular methods (PCR). All three patients died. All cases had a delay in definitive diagnosis that contributed to late treatment initiation and poor outcomes.
A comprehensive literature review of 34 studies from 1992–2025 highlights the diagnostic challenges and variable outcomes of M. genavense infection in individuals who are HIV-positive. PCR and 16S ribosomal RNA sequencing offer the highest diagnostic yield. Macrolide-based multidrug therapy remains the cornerstone of treatment, often requiring prolonged durations. Mortality rates range from 28.6–44.0%, and survival is significantly influenced by antiretroviral therapy adherence and timing of antimycobacterial therapy.
M. genavense should be considered in patients who are HIV-positive, especially those with CD4 less than 100 cells/µL and persistent constitutional symptoms and negative mycobacterial cultures. Terminal smear and PCR can play a pivotal role in diagnosing culture-negative disseminated infections. Empiric antimycobacterial therapy should be considered early in such patients, and diagnostic protocols should include terminal smear and molecular testing before treatment cessation. Early diagnosis and prompt initiation of treatment may improve outcomes in this vulnerable population.
Key Points
1.Mycobacterium genavense is a rare, fastidious non-tuberculous mycobacterium affecting patients with advanced HIV. Routine cultures often fail, delaying diagnosis and treatment. Recognising its clinical relevance is essential to improving patient outcomes.2.The authors present three fatal cases of M. genavense infection in advanced HIV, where diagnosis required terminal smear and PCR after repeated culture negativity. A literature review (1992–2025) contextualises these cases, highlighting diagnostic and therapeutic challenges.
3.In patients who are HIV-positive with cluster of differentiation (CD)4 <100 cells/µL and have persistent systemic symptoms with negative cultures, M. genavense should be suspected. Terminal smear and PCR are valuable diagnostic tools, and empiric antimycobacterial therapy should be initiated early to reduce delays and improve outcomes.
INTRODUCTION
Immunocompromised individuals are susceptible to mycobacterial infections. First identified in 1992, Mycobacterium genavense is a rare, slow-growing environmental non-tuberculous mycobacterium (NTM).1,2
M genavense has been identified in various sources, including tap water, the intestinal tracts of healthy humans, and several animals, such as birds, rabbits, cats, and ferrets.3 There is no evidence of human-to-human transmission. In birds, it is the most frequently isolated mycobacterium, particularly in parrots and parakeets.3-5
Laboratory identification of M. genavense infection is achieved through traditional acid-fast bacilli (AFB) smear microscopy of blood, lymphatic tissue, and bone marrow samples and culture methods, as discussed below in more detail.
The most traditionally used smear for AFB, a characteristic of Mycobacterium species, is the Ziehl–Neelsen stain. Auramine-phenol is increasingly used and more sensitive for AFB compared to Ziehl–Neelsen, which is more specific.6 Terminal smear refers to a smear, either Ziehl–Neelsen or Auramine, performed on culture-negative samples as a means of internal quality control. Terminal smear may be performed on blood, lymph node, and bone marrow samples. The terminal smear, although not a definitive diagnostic method, can provide an indication that mycobacteria are present, prompting further testing.7
The ideal medium for culturing M. genavense in primary cultures is Middlebrook 7H11, adjusted to an acidic pH of 6.2±0.2 and supplemented with charcoal and sheep blood. Under these conditions, all strains form colonies within 6–12 weeks, with colony counts nearly matching the initial bacterial inoculum.7,8 M. genavense requires liquid media, an acidic environment, elevated temperatures of around 45 °C, the addition of mycobactin J, and an incubation period of at least 3 months for successful growth. Due to its slow and challenging growth, molecular techniques are essential for definitive species identification. Additionally, susceptibility testing is particularly difficult because of its complex isolation process and the extended incubation time necessary for sufficient growth.7,9
In humans, infections can range from mild, nonspecific symptoms in otherwise healthy individuals to widespread disease in those who are immunocompromised. The clinical presentation closely resembles that of Mycobacterium avium complex infections, with symptoms and signs including fever, abdominal pain, diarrhoea, weight loss, lymphadenitis, hepatosplenomegaly, and progressive anaemia.10,11 Less frequently, the infection may involve the lungs, central nervous system, skin and soft tissues, or genital tract. Its affinity for the small intestine suggests that the digestive system could serve as a reservoir, with possible transmission occurring through oral or intestinal routes.12
Through examination of three cases managed in the unit, the authors highlight the role of terminal smear and molecular methods in diagnosing difficult-to-detect M. genavense infections in immunocompromised patients, showcasing its effectiveness in overcoming the limitations of conventional culture-based approaches.
CASE PRESENTATIONS
Case 1
Case 1 was a 44-year-old male who had a very late diagnosis of HIV-1 infection, complicated with Pneumocystis jirovecii pneumonia (PJP) and progressive multifocal leukoencephalopathy (PML). He was treated empirically for disseminated mycobacterial infection, but the diagnosis of M. genavense was only confirmed posthumously from in-house PCR of mycobacterial blood cultures.
The patient presented to hospital with new onset neurological deficit following a fall and head injury. Originally from Poland, he had no history of travel in the past 5 years and was living in the UK. He had no history of alcohol or recreational drug use, but smoked 20–30 pre-rolled cigarettes daily. He had exposure to cats and dogs and was married to a long-term male partner.
On admission, the patient exhibited isolated right lower limb weakness (Medical Research Council (MRC) scale 3/5 in all muscle groups), while right lower limb sensation remained intact. There were no other significant neurological deficits.
Initial diagnostic workup revealed that the patient was HIV-1 positive with cluster of differentiation (CD)4 82 cells/µL (7% absolute count). The patient was diagnosed with PJP and PML secondary to advanced HIV and initiated on high-dose co-trimoxazole for 21 days, along with antiretroviral treatment (ART) with emtricitabine and tenofovir disoproxil, and dolutegravir. As he had mild PJP, he did not receive steroids and was subsequently discharged home with appropriate outpatient follow-up.
The patient was re-admitted a week later with pyrexia and worsening neurology, having developed new confusion, left arm weakness, and hypotonia alongside pre-existing lower limb weakness. Serial blood cultures, sepsis screen, repeated lumbar puncture, and imaging failed to identify new sources of infection (Supplementary Table 1). Over the following 2 months, the patient continued to deteriorate with persisting fevers and became progressively comatose despite showing a virological response to ART. Serial blood cultures remained negative. In view of the persisting fevers, deranged liver function tests, and pancytopenia, he was eventually empirically treated for disseminated mycobacterial infection with clarithromycin 500 mg twice daily, ethambutol 800 mg once daily (OD), and rifabutin 300 mg OD. Rifabutin was chosen over rifampicin to avoid a clinically significant interaction that reduces dolutegravir concentrations.13 Additional consults were sought from neurology and haematology specialists, but, unfortunately, these did not offer new differentials. Pembrolizumab was considered for PML, but due to limited evidence and ongoing poor prognosis, it was felt that this would be unlikely to be beneficial. A summary of the clinical timeline and treatment received can be seen in Figure 1.
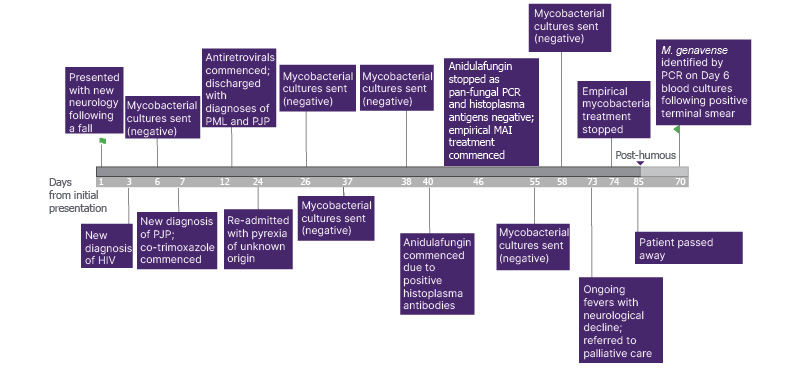
Figure 1: Timeline of case presentation and mycobacterial investigations highlighting difficulty in diagnosing M. genavense leading to delays in antimycobacterial treatment and poor prognosis (Case 1).
MAI: Mycobacterium avium-intracellulare; PJP: Pneumocystis jirovecii pneumonia; PML: progressive
multi-focal leukoencephalopathy.
Due to continued decline despite maximum treatment, the patient was referred to palliative care for end-of-life care. Medications were rationalised accordingly and antimycobacterial treatment was discontinued. He passed away 2 weeks later. As is standard practice in the local departmental mycobacteriology laboratory, a terminal AFB smear was performed on a culture-negative mycobacterial blood culture after 6-week incubation as part of routine in-house internal verification processes. In this case, microscopy was positive and prompted PCR, which identified M. genavense, suggestive of disseminated infection.
Case 2
Case 2 was a 36-year-old White British male with known advanced HIV infection (CD4: 30 cells/µL; 11% absolute count), whose treatment was complicated by episodes of disengagement from care and who was diagnosed with disseminated M. genavense infection by PCR on bone marrow aspirate, but relapsed 1 year later and ultimately passed away. He presented with widespread lymphadenopathy, fevers, pancytopenia, and significantly deranged liver function tests. CT scan of the thorax, abdomen, and pelvis showed multiple abdominal pathological lymph nodes with necrotic components. He underwent endoscopic ultrasound-guided biopsy of the necrotic nodes, which was sent for standard bacterial and fungal cultures as well as mycobacterial cultures ([hlFigure 2[/hl]). Lymph node samples were smear positive for AFBs, prompting commencement of azithromycin 500 mg OD, rifabutin 300 mg OD, and ethambutol 600 mg OD, pending organism identification. His ART was also restarted and, following this, he made a clinical recovery with defervescence of fevers and was discharged with outpatient follow-up.
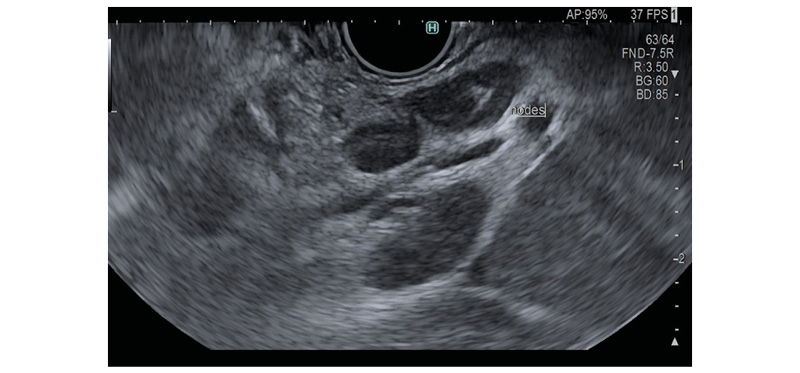
Figure 2: Endoscopic ultrasound of pathological necrotic abdominal nodes due to M. genavense (Case 2).
Multiple samples were culture-negative for mycobacteria after 8 weeks incubation on solid and liquid media. Due to the initial positive smear on the lymph node but negative culture, the Mycobacterial Growth Indicator Tube (MGIT) liquid from the smear-positive lymph node underwent PCR to confirm the initial smear-positive AFB results at the end of incubation. M. genavense was detected by PCR.
A year later, the patient presented with fevers and a first history of seizure following disengagement with HIV treatment. CT and MRI scans showed a solitary lesion within the right temporal lobe with surrounding oedema. He was commenced on treatment for suspected toxoplasmosis but showed no improvement after 2 weeks of treatment. Whole body CT was repeated and showed that the pathological lymph nodes remained unchanged. A summary of the investigations performed during this admission and their results can be viewed in Supplementary Table 2. The patient’s mycobacterial blood cultures remained negative by culture but positive on terminal smear and PCR for M. genavense.
Due to ongoing fevers, he was also managed empirically for neutropenic sepsis with high-dose piperacillin-tazobactam, until bacterial infection was excluded. His ART and anti-mycobacterial medication were also recommenced. Dieticians were also involved due to extreme malnutrition, and a supplementary nasogastric feeding regimen was recommended. Unfortunately, the patient declined medication and nutritional support. With the support of the inpatient psychiatry team, he was assessed as having capacity to make this decision. He self-discharged and unfortunately passed away a couple of weeks later, likely due to uncontrolled HIV, disseminated mycobacterial infection, and malnutrition.
Case 3
Case 3 was a 30-year-old man with vertically acquired HIV-1 infection who was admitted with pancytopenia and HIV wasting syndrome. First-line microbiological investigations were negative, and the diagnosis of disseminated NTM infection was made following positive AFB microscopy on bronchoalveolar lavage sample. However, multiple samples remained culture-negative, with the diagnosis of M. genavense infection being confirmed posthumously by PCR on both bronchoalveolar lavage samples and mycobacterial blood culture.
He presented with several weeks of progressive lethargy, profound fatigue, and worsening shortness of breath. He had a documented history of poor adherence to ART, marked by recurrent disengagement from care. He contacted his HIV care team due to escalating breathlessness and was subsequently admitted. On arrival, he appeared pale and malnourished, with a BMI of 17.3. Laboratory results revealed pancytopenia and severe immunosuppression, with a CD4 count of 1 cell/µL (1%) and an HIV viral load of 683,859 copies/mL. He required urgent transfusion for symptomatic anaemia (Supplementary Table 3).
On clinical examination, he was cachectic, with dry skin and bilateral pitting oedema. Cardiovascular and respiratory examinations were unremarkable. Abdominal examination revealed tenderness in the left upper quadrant, with percussion findings suggestive of splenomegaly. There was no oral candidiasis or peripheral lymphadenopathy; however, poor dentition was noted. Neurological examination was initially normal. He was commenced on combination ART with bictegravir/emtricitabine/tenofovir alafenamide and prophylactic treatment for opportunistic infections with fluconazole and co-trimoxazole. Due to persistent fever, he was empirically started on piperacillin–tazobactam and infection work-up commenced. A contrast-enhanced CT of the thorax, abdomen, and pelvis demonstrated hepatosplenomegaly with splenic infarcts and low-attenuation foci, diffuse subcutaneous oedema, ascites consistent with hypoalbuminaemia, and inflammatory pulmonary changes including bronchiectasis.
A diagnostic bronchoscopy was performed, yielding an AFB-positive smear. However, GeneXpert® (Cepheid, Sunnyvale, California, USA) Mycobacterium tuberculosis/rifampicin PCR and mycobacterial cultures were negative. Given ongoing pancytopenia, a bone marrow aspirate was obtained, revealing granulomatous inflammation. Microbiological cultures and PCR for mycobacteria, fungi, and other pathogens from the marrow were negative.
Considering these findings, empiric treatment for possible disseminated NTM infection was initiated with rifabutin 300 mg OD, ethambutol 800 mg OD, and azithromycin 500 mg OD. ART was subsequently adjusted to a regimen of dolutegravir and emtricitabine/tenofovir to mitigate potential drug–drug interactions with rifamycins.
He developed acute agitation without identifiable metabolic or structural cause and was too unsettled to undergo neuroimaging. He subsequently sustained a cardiac arrest. Despite full advanced life support measures and treatment of suspected reversible causes (including profound hyperkalaemia [K⁺ >8 mmol/L]), resuscitation efforts were unsuccessful after 40 minutes. Review of recent investigations showed no ECG abnormalities or corrected QT interval prolongation prior to the arrest.
Posthumously, the smear positive AFB from bronchoscopy was identified as M. genavense. Given his background, two mycobacterial blood cultures that were culture-negative on extended culture for 18 weeks underwent terminal smear and PCR, which also identified M. genavense. Other microbiological and infectious disease workup remained unremarkable and is summarised in Supplementary Table 3. The patient’s death was attributed to advanced HIV complicated by disseminated M. genavense infection and HIV wasting syndrome, with contributions from severe immunosuppression, malnutrition, and multisystem involvement.
LITERATURE REVIEW
Method
A local database of all M. genavense cases in Leeds Teaching Hospital Trust, UK, was searched, and these were the only three cases identified as of December 2024.
A search was conducted on PubMed and using Elicit Research Assistant (Elicit, Oakland, California, USA) to identify cases of M. genavense infection in patients with HIV in the literature. The PubMed search used the terms ‘Mycobacterium genavense’, ‘HIV’, and ‘Human Immunodeficiency Virus’. Elicit used the question ‘Literature Review of Reported Cases of Mycobacterium genavense in Immunocompromised Patients with HIV, 1992–2025’ to search across over 126 million academic papers from the semantic scholar corpus. Five hundred papers most relevant to the query were retrieved. Additional references were identified from citations within these papers. These studies were cross-referenced with the PubMed search outcomes and duplicates were removed.
- Studies were then screened and included if they met the following criteria:
- The study included patients with confirmed HIV infection
- M. genavense infection was confirmed through culture or molecular methods
- The study reported clinical presentation, diagnostic methods, and/or treatment outcomes
- The study design was a case report, case series, observational study, or systematic review
- Individual patient data could be extracted from the study
- The study involved human subjects rather than animal or in vitro experiments
- Published in English Language due to interpretive restrictions (non-English studies with English abstracts were reviewed, though the rest of the study in a different language was not appraised)
Results
A total of 33 publications, dated between 1992–2025, were identified through the search strategy. Including this present report, this yields a cumulative total of 34 reports reviewed in the literature. Of these, 19 are single-patient case reports, while the remainder consist of small case series, except for one meta-analysis encompassing 223 patients (171 who were HIV-positive and 52 who were HIV-negative; Supplementary Table 4).2
Two reports based on case series and retrospective observations reported frequency of symptoms, including fever in 75.0–87.0% and weight loss in 79.0–87.0% of cases;11,12 with other common findings of abdominal pain (71.0%),11 diarrhoea (44.0–62.5%),11,12 splenomegaly (43.0–71.0%),11,12 hepatomegaly (39.0–62.5%),11,12 lymphadenopathy (62.5%),11 and anaemia (72.0%).12
The analysis of the studies reviewed identified four main diagnostic methods for detecting M. genavense (Supplementary Table 4). Detection rates varied across these methods, with high detection rates reported for PCR14,15 and 16S rRNA sequencing,16,17 while culture using liquid media showed a low-to-moderate detection rate.18,19 AFB smear results were variable.20,21 No specific detection rates or quantitative comparisons between the methods were found. Some studies noted that the sensitivity of AFB smears may depend on the sample type and bacterial load. Culture using liquid media can be challenging due to the slow growth of M. genavense. PCR and 16S rRNA sequencing offer higher sensitivity and specificity, but may require specialised equipment. Additionally, line probe assays were suggested to show promise for more rapid and accurate identification of M. genavense, though further validation in larger studies is needed.15
The authors’ analysis of the included studies identified five antimicrobial classes used in the treatment of M. genavense infection: macrolides, rifamycins, ethambutol, fluoroquinolones, and aminoglycosides.12,16,17,20-24 Each antimicrobial class was reported in at least two studies, totalling 10 study reports across the five classes. Two reports note treatment courses of at least 12 months;12,25 one study observed median survival of 263 days for treated patients versus 81 days12 for untreated patients, and another reported overall mortality between 28.6–44.0% with a 1-year survival rate of 72%.11,26 Treatment duration varied significantly across studies, ranging from several months to over 2 years.12,24,25 More recent studies tend to report more standardised approaches to treatment, often based on macrolide-containing regimens. }The largest study reported high overall mortality, but found that macrolide-containing regimens were associated with better survival.2
The diverse range of infecting species and clinical presentations makes it challenging to generalise about the prognosis and mortality rates of NTM infections.10 However, evidence indicates that survival rates among individuals with HIV and NTM infections have significantly improved with the introduction of ART. For instance, a global case series from 1995, conducted before the availability of ART, found that 76% of 54 individuals with M. genavense infections and HIV had died within 1 year, with no survivors beyond 21 months (Table 1).10-12,25 In contrast, a retrospective study involving 25 cases of M. genavense infection in individuals with HIV, spanning 19 centres in France after ART became available, demonstrated significantly lower mortality rates: 26% at 1 year and 50% at 5 years.10-12
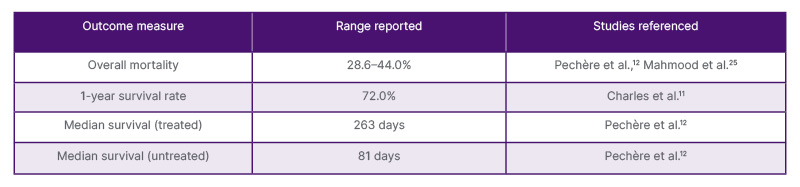
Table 1: Summary of literature on treatment response and outcomes in M. genavense infections.11,12,25
Outcomes are influenced by several factors, including the timing of diagnosis and treatment initiation, the patient’s underlying immune status and degree of immunosuppression, the presence of other opportunistic infections, and the use of highly active antiretroviral therapy in patients who are HIV-positive.27 Some studies report cases of relapse after initial treatment success, emphasising the need for prolonged therapy and close monitoring.28 While limited data exist on long-term outcomes, some studies suggest successful treatment with no relapse after extended follow-up periods.25 However, treatment challenges remain, as some studies document difficulties in eradicating the infection, with persistent positive cultures or clinical symptoms despite prolonged therapy.28
The authors reviewed all patients with HIV and disseminated NTM disease from their own unit. The authors identified nine patients with NTM and HIV infection between 2016–2023. The only three patients to have died were the patients with M. genavense infection described here. This highlights the potential poor prognosis that is associated with M. genavense, which may be, in part, due to delays in diagnosis.
DISCUSSION
In the cases presented in this report, conventional culture techniques initially yielded negative results, underscoring the limitations of culture-based diagnostics of M. genavense in immunocompromised individuals. PCR, however, was able to detect M. genavense DNA in various specimens, including blood and lymph tissue, allowing for a definitive diagnosis. In the first case, PCR testing would not have been conducted if the posthumous terminal smear had not been performed and yielded a positive result.
The first two cases suggest a potential role for terminal AFB smears in culture-negative samples, with follow-up PCR testing in patients identified as high risk for M. genavense infection. As all three cases highlight, delays in mycobacterial treatment lead to poor outcomes. Terminal smear refers to smear looking for AFBs performed on culture-negative samples, and is regarded as a quality control method rather than a definitive diagnostic procedure.
In a prospective study conducted between 1994–1995, 750 blood culture bottles submitted for mycobacteria detection between 1st January 1994–16th August 1995 were incubated for 12 weeks.9 These samples were noted to have been taken from mainly people living with advanced HIV (CD4 <50 cells/µL). They were reviewed after the incubation period, and 68 had a growth index (GI) >10, indicating mycobacterial presence. Among 545 negative cultures (GI <10) over 12 weeks, Ziehl-Neelsen staining detected AFB in one, later identified as M. genavense via hsp65 PCR analysis. In six of 39 patients with positive cultures, growth occurred after more than 6 weeks (M. tuberculosis in one, M. genavense in three, and Mycobacterium avium complex in two). The conclusion of this study was that, though extended incubation and systematic Ziehl-Neelsen staining increased M. genavense recovery from 5.0% to 14.5%, only three patients received antimycobacterial treatment due to late detection.9
Even though the terminal smear can be useful, it is typically less sensitive than more specialised methods like PCR or 16s rRNA sequencing. While the terminal smear may reveal the presence of AFB, it cannot differentiate between various species of mycobacteria. In some cases, the smear may be negative, especially if the bacterial load is low, as may be seen in disseminated infections in the immunocompromised.9 The authors’ local standard operating procedure for identification of mycobacterial species follows a process of DNA extraction, amplification, and sequencing using 16S. In-depth mycobacterial analysis requires dedicated scientists and specialist equipment, which may only be available in specialised laboratories, and given that disseminated M. genavense is a rare disease, widespread application of these methods may not be practical.
Despite its advantages, as described in this report and the literature, PCR can occasionally yield false positive results or fail to distinguish between M. genavense and other closely related mycobacterial species. Cross-reactivity with other NTM species is a known issue, and further sequence analysis or specific probes may be required to confirm the species identity. Additionally, PCR can only detect the presence of bacterial DNA and does not provide information on the viability of the bacteria, which is important for understanding the clinical significance of the result.5,9
PCR may be performed on various sample types, including blood, tissue, fluid, and stool; however, there is no direct comparison in sensitivity and specificity of PCR of these different methods, and generally diagnosis of disseminated NTM in HIV infection requires a positive blood culture. There is no role for screening or early surveillance for disseminated NTM infections, as the investigations described are clinical diagnostic tests as opposed to screening tests. However, in patients presenting with a consistent clinical syndrome and CD4 <100 cells/µL, it is important to send at least two mycobacterial blood cultures and consider mycobacterial PCR if appropriate and locally available.
The diagnostic accuracy of quantitative PCR on stool has been investigated in M. tuberculosis complex, and results show it has comparable sensitivity to sputum Xpert® Ultra (Cepheid, Sunnyvale, California, USA; 94.8%; 89.1–98.1), and, thus, may be a valuable tool for the diagnosis of tuberculosis, particularly in patients unable to produce sputum, which is often the case in advanced HIV.29 However, the role of stool PCR for the diagnosis of disseminated NTM is not well understood, and there may be difficulties with low bacterial load and the presence of PCR inhibitors in stool, such as bile salts, haem, and polysaccharides, both resulting in false negative results.
The UK Standard for Microbiological Investigations (UK SMI) describes the role of real-time PCR in diagnosing M. tuberculosis infections and genetic mutations associated with drug resistance.7 Commercially available DNA line probe assays, which are sensitive and specific for identifying most mycobacteria, are available but limited due to misidentification of different strains such as Mycobacterium abscessus and Mycobacterium chelonae. At the time of writing, there is no recommendation in the UK SMI for routine terminal smears or PCR in culture-negative mycobacterial samples.7
CONCLUSION
The authors’ findings are consistent with previous studies that have shown the difficulty in diagnosing infections caused by difficult-to-grow mycobacteria. In suspected disseminated mycobacterial infection, empiric treatment should be considered in patients with compatible symptoms and signs after appropriate cultures have been taken, and treatment should not be discontinued prematurely whilst awaiting culture results. While culture remains gold-standard, consideration should be given to terminal smear, PCR (if terminal smear is positive), and histopathology to allow a timelier diagnosis and reduce delays in commencement of appropriate therapy if treatment has not been started empirically. The authors’ case series and literature review highlight the significant morbidity and mortality associated with disseminated M. genavense infection, thus timely diagnosis and treatment are of utmost importance. The case series and current local practice suggest that terminal smear and PCR could be considered as part of a standardised diagnostic pathway on all samples from patients with suspected disseminated mycobacterial infection and advanced HIV infection (CD4 <100 cells/µL) before stopping empiric treatment if cultures are negative.




