Abstract
Background: Fetal anaemia is a serious obstetric complication associated with high perinatal morbidity and mortality, most commonly resulting from maternal red cell alloimmunisation or parvovirus B19 infection. Intrauterine blood transfusion (IUT), performed using a fine needle under continuous ultrasound guidance to deliver blood directly into the fetal circulation, most commonly through the umbilical vein at its placental insertion or via the intrahepatic portion, has revolutionised the management of fetal anaemia. In Ethiopia, Rh alloimmunisation remains relatively common, affecting 9.8–17.1% of RhD negative pregnant women; however, data on fetal anaemia prevalence are lacking.
Case presentation: A 28-year-old G4P2A1 from Addis Ababa, Ethiopia, was referred to Abebech Gobena Mothers and Children’s Health Hospital at 19 weeks gestation with Rh isoimmunisation: her blood group was O negative, while her partner’s blood group was O positive. Her history included one live birth, one miscarriage, and one stillbirth. The indirect Coombs test was positive, and weekly fetal surveillance using middle cerebral artery (MCA) Doppler was initiated. The first IUT was performed at 21 weeks when the MCA peak systolic velocity reached 1.577 multiple of the median. Fetal blood group and Rh (3rd IUT) was O positive; Direct Coombs test was not performed due to unavailability. Serial transfusions followed, with a total of 10 IUTs completed, the final one at 37 weeks. The decision to perform each IUT was based on elevated MCA peak systolic velocity multiples of the median values, indicating ongoing or recurrent fetal anaemia. At 38 weeks, a male neonate weighing 3,500 g was delivered via Caesarean section with Apgar scores of 9 and 10 at 1 and 5 minutes, respectively. Postnatal assessment showed normal haematologic and bilirubin levels and normal echocardiography, with no need for exchange transfusion or phototherapy. Both mother and neonate were discharged in good condition.
In this case, the decision to proceed with IUT beyond 34 weeks gestation was based on an individualised assessment of risks and benefits, as delivery at 34 weeks in the setting of a limited NICU facility was assessed to carry a higher risk of neonatal morbidity and mortality than continuation of pregnancy following fetal stabilisation. Accordingly, a deliberate fetal protective approach was adopted to optimise fetal survival and minimise overall risk, including the need for emergency neonatal resuscitation.
Conclusion: This case demonstrates that late IUT performed at 37 weeks, followed by delivery at term (38 weeks), can result in a favourable neonatal outcome without the need for postnatal interventions. When conducted in experienced centres, late intrauterine transfusion appears to offer a promising strategy for improving outcomes in severely isoimmunised pregnancies.
Key Points
1. Fetal anaemia from Rh alloimmunisation remains a significant contributor to perinatal morbidity and mortality, particularly in low resource settings like Ethiopia, where prevalence among RhD negative pregnancies remains high.
2. This case report describes a 28-year-old multiparous woman with Rh isoimmunisation managed through 10 intrauterine transfusions, including late intervention at 37 weeks gestation.
3. Carefully selected late intrauterine transfusion beyond 34 weeks, guided by fetal monitoring and contextual resource considerations, may safely optimise neonatal outcomes and reduce the need for preterm delivery and postnatal interventions.
INTRODUCTION
Haemolytic disease of the fetus occurs when there is red blood cell (RBC) incompatibility between a pregnant women and their fetus. This condition arises when maternal alloantibodies cross the placental barrier in sufficient quantities and bind to specific antigens on the surface of fetal RBCs, leading to fetal haemolysis and anaemia.1,2
Fetal anaemia is a significant obstetric complication that can lead to considerable perinatal morbidity and mortality. The most frequent aetiologies are maternal alloimmunisation and infection with parvovirus B19.3,4 Intrauterine transfusion (IUT) has revolutionised the management of fetal anaemia, and is performed using a fine needle under continuous ultrasound guidance to deliver blood directly into the fetal circulation, most commonly through the umbilical vein at its placental insertion or via the intrahepatic portion.5,6
A study conducted at Wolaita Sodo University, Ethiopia, reported that 12.08% of pregnant women were RhD-negative. Among these women, 9.8% were found to be alloimmunised, indicating that approximately one in 10 RhD-negative pregnant women had developed alloantibodies.7 Similarly, research carried out at Addis Ababa University revealed that the prevalence of RhD negativity and Rh alloimmunisation was 2.1% and 17.1%, respectively. These findings highlight a relatively high rate of alloimmunisation, with nearly one in five RhD-negative pregnant women affected.8
ETHICAL REVIEW
Institutional approval was obtained both for the study of the case and for the publication of this case report, in accordance with institutional guidelines. Approval was granted by the Institutional Review Board (IRB) of Yekatit 12 Hospital Medical College (Y12HMC). Written informed consent for publication of this case report and any accompanying images was obtained from the mother involved in the case.
CASE REPORT
A 28-year-old G4P2A1 mother from Addis Ababa, Ethiopia, was referred from a local health centre to Abebech Gobena Hospital with a diagnosis of Rh isoimmunisation at 19 weeks of gestation. Her blood group was O negative, while her partner’s blood group was O positive. Her first pregnancy resulted in a healthy vaginal delivery 4 years ago. The second pregnancy ended in a miscarriage at 8 weeks of gestation, and the third resulted in a stillbirth at 32 weeks for unknown reasons. Evaluation at the maternal fetal medicine unit showed a positive indirect Coombs test; Coombs titration was not performed due to limited resources. Fetal anatomy was normal on ultrasound, and serial assessments of the middle cerebral artery (MCA) peak systolic velocity (PSV) were conducted.
The mother was followed for 2 weeks, and the first intrauterine transfusion was performed at 21 weeks when the MCA Doppler PSV reached 42.11 cm/s (1.577 multiples of the median [MoM]), as shown in Figure 1. The initial transfusion was carried out via the transperitoneal route, followed by a second IUT at 22 weeks and 3 days, and on follow-up 1 week later, the previously transfused peritoneal blood had been completely absorbed.
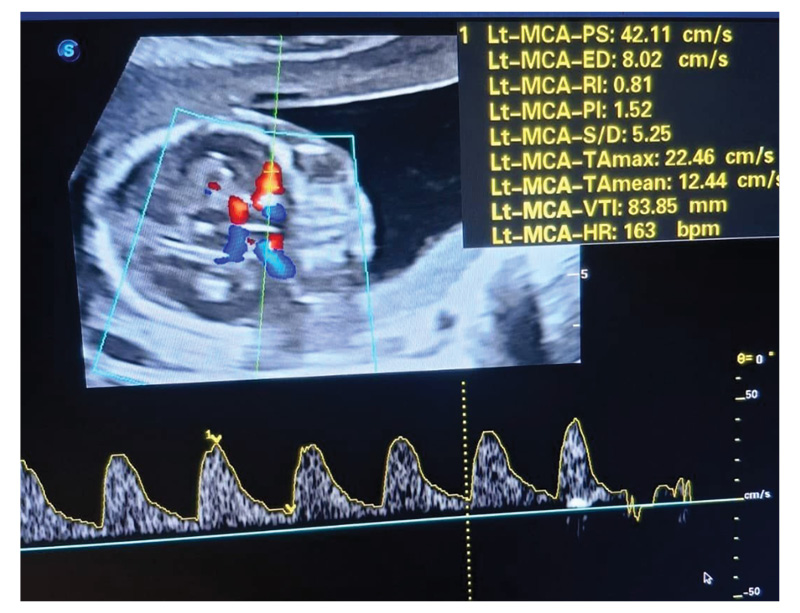
Figure 1: MCA Doppler ultrasound at 21 weeks of gestation showing a peak systolic velocity of 42.11 cm/s, corresponding to 1.577 MoM.
MCA: middle cerebral artery; MoM: multiples of the median.
At 25 weeks and 3 days of gestation, new onset minimal fetal ascites was detected and MCA Doppler was 2.0 MoM, as shown in Figure 2. A third IUT was then performed intravascularly through the umbilical vein at the placental cord insertion site, as shown in Figure 3. The pretransfusion haemoglobin and haematocrit levels were 5.5 g/dL and 14.5%, respectively. Fetal blood group and Rh were O positive; the Direct Coombs test was not performed due to unavailability.
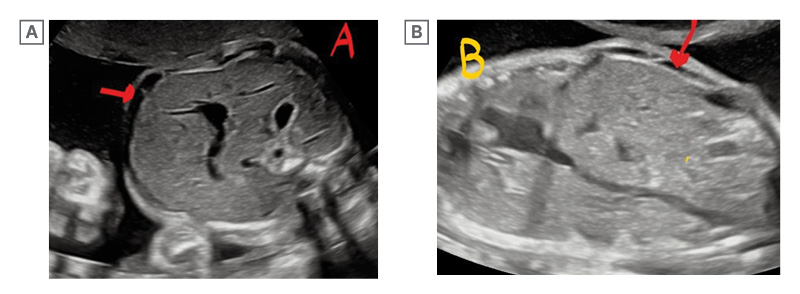
Figure 2: Ultrasound sonogram at 25 weeks and 3 days of gestation showing fetal ascites (red arrow) in both transverse (A) and longitudinal (B) views.
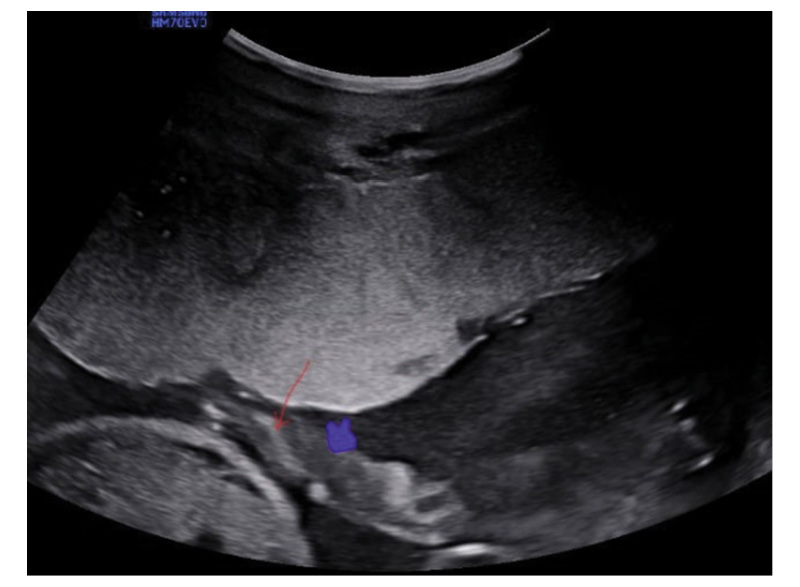
Figure 3: Sonogram illustrates an intrauterine blood transfusion through intravascular access at the placental insertion site of the umbilical cord. The red arrow highlights the transfused blood jet, and the blue arrowhead marks the umbilical vein wall.
The procedure was continued, with the tenth and final IUT conducted at 37 weeks gestation. The decision to perform each IUT was based on elevated MCA-PSV MoM values, indicating ongoing or recurrent fetal anaemia. A male infant weighing 3,500 g was delivered via Caesarean section at 38 weeks, with Apgar scores of 9 and 10 at 1 and 5 minutes, respectively. Postnatal haematocrit was 38.1%, haemoglobin 15.1 g/dL, and bilirubin levels were 1.7 mg/dL (direct) and 0.7 mg/dL (indirect). Echocardiography was normal. The neonate required no exchange transfusion or phototherapy and was supported with 2 L nasal continuous positive airway pressure for oxygen saturations of approximately 86–90%, which improved progressively without further intervention. After 1 week of observation and stable follow-up, he was discharged in good condition. Details of the IUT are summarised in Table 1.
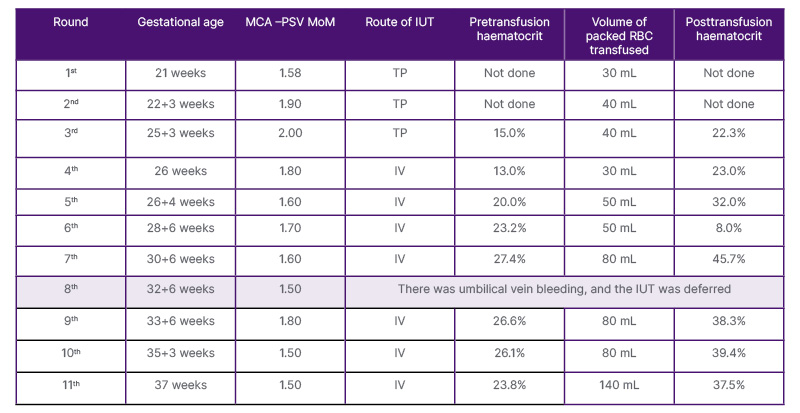
Table 1: Summary of intrauterine transfusion procedures.
The required transfusion volume was determined using the Fetal Medicine Foundation online fetal anaemia calculator.
IUT: intrauterine transfusion; IV: intravenous; MCA-PSV: middle cerebral artery peak systolic velocity; MoM: multiples of the median; RBC: red blood cell; TP: transperitoneal.
DISCUSSION
To the best of the authors’ knowledge, this is the first reported case in Africa and the second worldwide following the case reported in Rio de Janeiro, Brazil, in which a fetus successfully underwent 10 intrauterine transfusion cycles and was delivered alive.9
IUT is commonly the treatment of choice for severe cases of Rh alloimmunisation, effectively preventing intrauterine death and achieving fetal survival rates of 60–90%.10-12 However, the procedure is not without risk. IUT can promote the passage of fetal blood into the maternal circulation, potentially exacerbating the maternal immune response. Additional complications include hypercapnia, bradycardia, premature rupture of membranes, and umbilical cord bleeding, which can occasionally result in fetal death.13 In the authors’ case, umbilical cord bleeding occurred during the eighth intrauterine transfusion, necessitating the temporary discontinuation of the procedure; the IUT was repeated 7 days later and was successfully completed.
In a single centre study at Leiden University Medical Center, the Netherlands, 254 fetuses underwent 740 intrauterine transfusions for maternal red cell alloimmunisation. The overall survival rate was 89%, with procedure-related complications at 9% (3.1% per procedure) and perinatal loss at 4.7% (1.6% per procedure).14 Similarly, at Kanuni Sultan Suleyman Research and Training Hospital in Istanbul, Türkiye, 110 intrauterine transfusions were performed in 42 fetuses, with a post-transfusion survival rate of 80.95% and procedure-related complications in 12.7% of cases.15
A 5-year retrospective study conducted at St. Paul’s Hospital Millennium Medical College (SPHMMC), Ethiopia, found that among 21 fetuses who required intrauterine transfusion, the average number of transfusions per fetus was two, with a maximum of six transfusions administered to a single case. Nine cases (42.85%) received one transfusion. The earliest gestational age at the first IUT was 24+4/7 weeks, while the latest was 35 weeks. In most cases (61.9%), the IUT was performed between 29 and 33 weeks of gestation. Among the 20 live born neonates, all received phototherapy, and 15 (75%) required exchange transfusion.16
A case from Rio de Janeiro, Brazil, describes a neonate born to a 29-year-old woman who underwent 10 intrauterine transfusions starting at 21 weeks gestation for perinatal haemolytic disease. The male infant was delivered by Caesarean section at 34 weeks and 2 days, weighing 2,540 g. He developed respiratory distress managed with nasal continuous positive airway pressure, and received phototherapy, exchange transfusion, and immunoglobulin. Supraventricular tachycardia was treated with vagal manoeuvres and amiodarone. The infant was discharged in good condition after 13 days.9
Extending IUT beyond 34 weeks in selected cases appears safe and is associated with improved obstetric and neonatal outcomes. This approach did not result in an increase in procedure related complications and was linked to higher mean gestational age at delivery, increased birth weights, and reduced rates of NICU admission.17-20
In this case, the decision to proceed with IUT beyond 34 weeks gestation was based on an individualised assessment of risks and benefits, as delivery at 34 weeks in the setting of a limited NICU facility was assessed to carry a higher risk of neonatal morbidity and mortality than continuation of pregnancy following fetal stabilisation. Accordingly, a deliberate fetal protective approach was adopted to optimise fetal survival and minimise overall risk, including the need for emergency neonatal resuscitation. Late IUT, particularly when performed close to delivery, gradually corrects fetal anaemia, avoids abrupt haemodynamic shifts, improves immediate postnatal adaptation, and reduces the likelihood of postnatal exchange transfusion, thereby lowering the risks of intraventricular haemorrhage, necrotising enterocolitis, pulmonary hypertension, metabolic acidosis, and infection.
CONCLUSION
This single case experience demonstrated that late intrauterine transfusion performed at 37 weeks, followed by delivery at term (38 weeks), resulted in a favourable neonatal outcome, with no need for phototherapy or exchange transfusion. Late intrauterine transfusion, when performed in centres with substantial experience and expertise, appears to have the potential to improve the prognosis of severely isoimmunised fetuses.






