BACKGROUND AND AIMS
Interstitial lung disease (ILD) is associated with progressive, debilitating symptoms, and hospitalizations occur frequently, with a report from the Pulmonary Fibrosis Foundation registry that described 34.7% of patients with ILD were hospitalized between March 2016–May 2021.1 Although respiratory-related hospitalizations were associated with poor clinical outcomes, post-discharge use of pulmonary rehabilitation (PR) was not reported. In other chronic respiratory disorders, such as COPD, PR after hospital discharge is associated with reduced healthcare use and improved patient outcomes.2 However, there is limited data concerning post-hospital discharge use of PR in patients with ILD, and the aim of this study was to assess the use of PR at the population level for post-hospital discharge patients with ILD in the United States.3
MATERIALS AND METHODS
The authors used IBM MarketScan® Research Database (Merative, Ann Arbor, Michigan, USA) to identify adults hospitalized with idiopathic pulmonary fibrosis (IPF) or non-IPF ILD between January 1, 2014–December 31, 2023. PR use was defined as identification of ≥1 claim within 3 months after hospital discharge and excluded patients with neuromuscular conditions, dementia, or discharge to a skilled nursing facility, long-term acute care hospital or hospice.
RESULTS
Among 11,413 eligible patients, 548 (4.8%) participated in PR within 90 days of hospital discharge (Figure 1). PR participants had a mean age of 62.9±11.0 years, which was similar to patients who did not participate in PR. Greater PR participation was noted in males, prior oxygen prescription, antifibrotic use, PR participation in the previous 12 months, and lung transplantation or evaluation in the previous 12 months. Logistic regression model revealed male sex and prior oxygen prescriptions were associated with higher odds of PR utilization, while factors associated with a lower likelihood of PR utilization included greater comorbidities and, in the preceding 12 months, no prior lung transplant surgery or transplant evaluation. Prior prescriptions for antifibrotics or immunosuppressive therapy were not associated with PR participation. Of note, patients with IPF participated in more than eight PR sessions more often compared to patients with non-IPF-ILD.
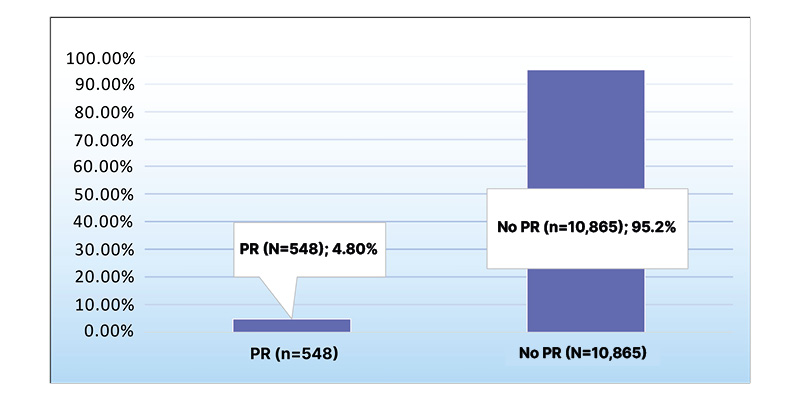
Figure 1: Frequency of pulmonary rehabilitation use 90 days after hospital discharge in patients with interstitial lung disease.
PR: pulmonary rehabilitation.
CONCLUSION
In conclusion, PR utilization after hospital discharge for patients with IPF and non-IPF ILD was low, and factors associated with increased PR included males and patients with prior oxygen prescription.






