BACKGROUND AND AIMS
Fungal infections are a frequent and clinically important complication after lung transplantation. Lung transplant recipients are uniquely vulnerable because the allograft is directly exposed to the external environment.1,2 In addition, airway instrumentation and structural lung disease may further increase susceptibility to fungal colonization and invasive fungal infection. Aspergillus and Candida species account for most fungal infections in this population, although mucormycosis, endemic fungi, and Pneumocystis jirovecii may also occur depending on host factors, prophylaxis practices, and local epidemiology.2-4
The relationship between post-transplant fungal infection and patient centered outcomes remains incompletely defined in large, real-world, multicenter cohorts. The authors aimed to evaluate the association between post-transplant fungal infection and mortality, allograft rejection, and chronic lung allograft dysfunction (CLAD) among adult lung transplant recipients.5
MATERIALS AND METHODS
The authors conducted a retrospective cohort study using the TriNetX Global Collaborative Network (TriNetX, LLC, Cambridge, Massachusetts, USA), which captures de-identified data from >160 healthcare organizations across North America, Europe, and Asia. Adult lung transplant recipients (≥18 years) between 2005–2024 were identified using International Classification of Diseases, 10th Revision (ICD-10) and Current Procedural Terminology (CPT®) codes. Patients with post-transplant fungal infection (aspergillosis, candidiasis, mucormycosis, histoplasmosis, coccidioidomycosis, blastomycosis, and pneumocystosis) and matched controls without fungal infection, within 1 year before or any time after transplant, were identified. The index date was defined as the date of lung transplantation.
Propensity-score matching was performed across demographics, comorbidities, laboratory values, procedures, and immunosuppressive medications. Outcomes included all-cause mortality, allograft rejection, and CLAD at 6 months and 1 year. Kaplan–Meier analysis and Cox proportional hazards models were used to estimate risk ratios (RR), hazard ratios, and 95% CIs. Analyses were conducted using TriNetX Analytics version 25.0 (TriNetX, LLC, Cambridge, Massachusetts, USA).
RESULTS
A total of 3,083 patients with post-transplant fungal infection and 11,625 patients without fungal infection were identified. The mean age was 58±13 years, and 56% were male. The most common pulmonary comorbidities were COPD, unspecified pulmonary fibrosis, and bronchiectasis. After propensity-score matching across 56 clinical variables, 1,790 patients remained in each cohort. Mortality was significantly higher in the fungal infection cohort, occurring in 13% versus 9% at 6 months (RR: 1.45; 95% CI: 1.20–1.75; p=0.001) and 17.8% versus 13% at 1 year (RR: 1.36; p=0.0001). Allograft rejection was more frequent among patients with fungal infection, occurring in approximately 46 compared with 22 among matched controls at 6 months. CLAD occurred approximately two- to three-fold more frequently in the fungal infection cohort compared with the non-infected cohort (Table 1).
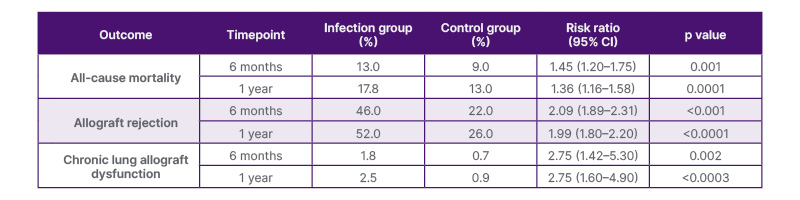
Table 1: Outcomes in propensity score-matched cohorts (n=1,790 per group).
Values shown represent cumulative incidence at each timepoint.
DISCUSSION
In this large, multicenter, propensity-matched analysis, post-transplant fungal infection was associated with significantly worse outcomes, including higher all-cause mortality, increased allograft rejection, and CLAD.
Fungal organisms may cause direct airway and parenchymal injury, particularly in the setting of impaired mucociliary clearance. Infections may amplify local inflammation and promote epithelial injury, which increases susceptibility to acute rejection. In turn, recurrent injury and inflammation may contribute to CLAD.1,6 The observed two- to three-fold higher risk of CLAD among patients with fungal infection suggests that fungal surveillance and prevention strategies may have implications beyond short-term infection control.3 Although propensity-score matching reduces measured confounding, residual confounding by disease severity, center-level prophylaxis and diagnostic practices, timing of infection, antifungal exposure, and distinction between colonization and invasive infection remains possible.
CONCLUSION
Post-transplant fungal infection was independently associated with increased mortality, allograft rejection, and CLAD among lung transplant recipients. These findings highlight the need for optimized surveillance, prophylaxis, and individualized post-transplant management strategies.