BACKGROUND AND AIMS
Sepsis is a life-threatening condition associated with significant morbidity and mortality.1 Decubitus ulcers (pressure injuries) are common in hospitalized patients and may become a source of infection.2,3 Pressure injuries may become complicated by local infection, osteomyelitis, bacteremia, and sepsis.4 This study seeks to investigate the association between the presence of decubitus ulcers and inpatient outcomes, including mortality, resource utilization, and complications, among patients hospitalized with sepsis in the United States, as large-scale data on this association are limited.5
MATERIALS AND METHODS
This retrospective cohort study utilized the Nationwide Inpatient Sample (NIS) database from 2016–2021. Patients hospitalized with a primary diagnosis of sepsis were identified and stratified based on the presence or absence of a concurrent diagnosis of decubitus ulcer. Multivariable logistic regression was used to assess the odds of in-hospital mortality and specific complications (severe sepsis, septic shock, disseminated intravascular coagulation, acute respiratory distress syndrome, mechanical ventilation, and acute kidney injury). Multivariable linear regression was used to compare total hospital charges, costs, and length of stay (LOS). Models were adjusted for patient demographics (age, gender, race, income quartile, and insurance), the Charlson Comorbidity Index, patient residence location, and hospital characteristics (region, bed size, and teaching status).
RESULTS
Of approximately 13.1 million weighted sepsis admissions, 1,046,110 (8.0%) had comorbid decubitus ulcers (2016–2021; (Figure 1)). Patients with decubitus ulcers were slightly older (mean age: 64.5 versus 69.3 years; p<0.01) and had higher comorbidity burdens. After multivariable adjustment, the presence of a decubitus ulcer was significantly associated with 35% increased odds of in-hospital mortality (1.35; p<0.01). Decubitus ulcers were also associated with significantly higher adjusted total hospital charges (40,776.83 USD; p<0.01), total costs (8,175.51 USD; p<0.01), and longer LOS (3.85 days; p<0.01). Furthermore, decubitus ulcers were associated with significantly higher adjusted odds of developing severe sepsis (adjusted odds ratio [AOR]: 1.35), septic shock (AOR: 1.58), disseminated intravascular coagulation (AOR: 1.18), requiring mechanical ventilation (AOR: 3.99), and acute kidney injury (AOR: 1.05; all p<0.01). No significant association was found with acute respiratory distress syndrome (AOR: 1.04; p=0.068).
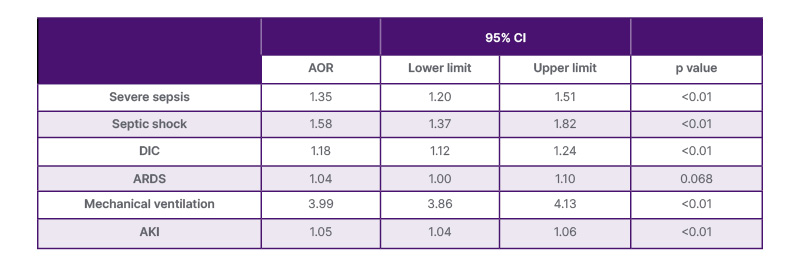
Table 1: Adjusted odds ratio of complications comparing teaching versus non-teaching hospitals.
p<0.05 indicates statistical significance. Multivariable regression models were adjusted for age at admission, gender, race, median household income national quartile for patient ZIP Code, Charlson Comorbidity Index, location/teaching status of the hospital, region of the hospital, patient’s residence, and insurance.
AKI: acute kidney injury; ARDS: acute respiratory distress syndrome; DIC: disseminated intravascular coagulation.
CONCLUSION
The study suggests the presence of a decubitus ulcer was independently associated with significantly increased inpatient mortality, higher resource utilization (cost, LOS), and greater odds of major sepsis-related complications. These findings, with similar results to prior literature6 highlight decubitus ulcers as an important indicator of adverse outcomes in patients with sepsis, emphasizing the need for targeted prevention and management strategies in this vulnerable population.