Meeting Summary
Biologics represent important treatment options for COPD and asthma, targeting inflammatory cytokines involved in the underlying disease pathophysiology. Dupilumab is a fully human monoclonal antibody (mAb) that blocks the shared receptor component for IL-4 and IL-13, key and central drivers of Type 2 inflammation, and is approved in the USA for the treatment of COPD and asthma as well as atopic dermatitis, chronic rhinosinusitis with nasal polyps, eosinophilic esophagitis, prurigo nodularis, chronic spontaneous urticaria, bullous pemphigoid, and allergic fungal rhinosinusitis. Itepekimab, an investigational mAb targeting IL-33, is undergoing clinical evaluation as a potential treatment for COPD and other respiratory diseases. This article summarizes data from a selection of poster and oral presentations on dupilumab and itepekimab in COPD and asthma disclosed during the 2026 American Thoracic Society (ATS) International Conference.
In COPD, Simon Couillard from the University of Sherbrooke, Canada, presented a post-hoc analysis of the pivotal BOREAS and NOTUS trials, showing that dupilumab reduced exacerbations and improved lung function versus placebo, irrespective of the degree of airway damage at baseline, with a greater magnitude of exacerbation reduction and greater lung function improvement among patients with less airway damage. This suggests additional clinical benefits with earlier dupilumab treatment when lung function impairment is less pronounced and lung damage remains more reversible. Findings from a causal mediation analysis, disclosed by Surya Bhatt from the University of Alabama at Birmingham, USA, demonstrated that patient-reported outcome (PRO) improvements with dupilumab were mediated by a combination of reduction in exacerbation frequency, improvement in lung function, and declines in fractional exhaled nitric oxide (FeNO) levels. Bhatt also presented study design details for the ongoing multinational Phase IV AEOLUS trial in patients with COPD and Type 2 inflammation, which will use lung imaging to evaluate the effect of dupilumab on airway inflammation and remodeling, including mucus plugging. Within the wider biologic space, Klaus Rabe from Christian-Albrechts University in Kiel, Germany, and Fernando Martinez from the University of Massachusetts, USA, discussed data on the efficacy and safety of itepekimab in former smokers with COPD from the pivotal Phase III AERIFY-1 and AERIFY-2 trials.
In the asthma arena, Guy Brusselle from Ghent University Hospital, Belgium, presented results from a post-hoc analysis showing that patients who achieved clinical remission with dupilumab in the pivotal QUEST trial were more likely to remain in remission in the long-term TRAVERSE extension study. Finally, Mona Al-Ahmad from Kuwait University, Kuwait, showcased data from an analysis of QUEST and TRAVERSE, demonstrating the long-term efficacy of dupilumab in patients with asthma and coexisting Type 2 inflammatory conditions.
New Data for Dupilumab In COPD
COPD is characterized by progressive damage to the lungs and airways, leading to airflow obstruction, chronic respiratory symptoms, and an increased risk of exacerbations.1 In the Phase III BOREAS and NOTUS trials, add-on dupilumab significantly reduced moderate or severe exacerbations and improved lung function, symptoms, and quality of life (QoL) versus placebo in patients with COPD and Type 2 inflammation.2-5
BOREAS (NCT03930732) and NOTUS (NCT04456673) were both Phase III, randomized, double-blind, placebo-controlled trials that enrolled patients aged 40–85 years with COPD and Type 2 inflammation (screening blood eosinophil counts≥300 cells/μL) on inhaled triple therapy. Patients received dupilumab 300 mg every 2 weeks (q2w) or matching placebo for a total treatment period of 52 weeks.2-5
Impact of Airway Damage and Disease Activity on Dupilumab Effects
Impaired lung function in patients with COPD is known to be associated with a higher risk for disease exacerbations. The opportunity for treatment is therefore greatest before advanced structural lung damage arises, particularly when inflammatory activity is high.6-8 Early identification and intervention in COPD were also key themes in the updated 2026 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, which emphasize modifiable biological activityand encourage clinicians to treat early toslow disease progression beyondsymptom control.9,10
Against this backdrop, post-hoc analysis of the BOREAS and NOTUS trials was undertaken to assess whether airway damage (estimated by baseline post-bronchodilator percent predicted forced expiratory volume in 1 second [ppFEV1]) and disease activity (indicated by Type 2 biomarkers) interactto predict future exacerbation risksand lung function decline in dupilumab-treated patients.11
Annualized moderate or severe exacerbation rates and change from baseline to Week 52 in pre- and post-bronchodilator FEV1 were measured in patients with baseline post-bronchodilator ppFEV1 ≤60% and >60%. In patients with baseline biomarker data, continuous spline regression (stratified by baseline post-bronchodilator ppFEV1 ≤40%, >40% to ≤60%, and >60%) was also usedto assess:
- Adjusted annualized exacerbation rates by baseline FeNO and blood eosinophil count
- Change from baseline in post-bronchodilator FEV1 at Week 52 by baseline FeNO
In total, 1,726 patients were included in this post-hoc analysis, 861 treated with dupilumab and 865 in the placebo arm.11
Results showed that dupilumab treatment was associated with greater reductions in moderate or severe exacerbation rates and lung function improvement compared to placebo, regardless of airway damage at baseline. However, patients receiving dupilumab who had less airway damage at baseline experienced a greater magnitude of exacerbation reduction during the trial, as well as lung function improvement at Week 52 versus placebo (Figure 1). In both arms, patients with baseline post-bronchodilator ppFEV1 ≤40% experienced more exacerbations than those with ppFEV1 of 40–60% or >60%.11
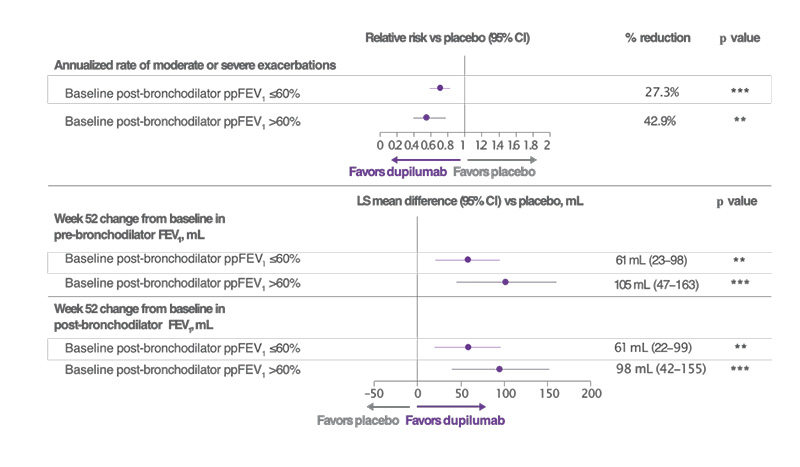
Figure 1: Patients receiving dupilumab versus placebo, and who had less airway damage at baseline, had a greater magnitude of exacerbation reduction during the trial as well as lung function improvement at Week 52.11
***p<0.001
**p<0.01 vs placebo
ppFEV1 <60%: dupilumab, n=720; placebo, n=693. ppFEV1 >60%: dupilumab, n=215; placebo, n=242.
LS: least squares; ppFEV1: percent predicted forced expiratory volume in 1 second; vs: versus.
In terms of biomarker interactions, reductions in moderate or severe exacerbations occurred in dupilumab-treated patients versus placebo, with a greater magnitude of reduction observed in patients with higher baseline FeNO or eosinophil count. Continuous spline regression also indicated that dupilumab versus placebo improved post-bronchodilator FEV1 at Week 52, with significantly greater lung function improvements seen in patients with higher baseline FeNO and eosinophil levels (interaction p=0.049).11
Overall, findings from this post-hoc analysis showed that dupilumab reduced exacerbations and improved lung function, regardless of the degree of airway damage at baseline. However, patients with better preserved lung function at the start of the treatment period had greater improvements compared with patients with advanced airway damage at baseline, as did patients with higher 2-type biomarker levels.11
Starting treatment with dupilumab earlier in the disease course, when lung function impairment is smaller and lung damage has a greater reversible component, may therefore result in better therapeutic outcomes than initiating treatment later, especially in patients with more active disease.11 This approach is aligned with updated GOLD guidelines in COPD, which emphasize the importance of early targeted intervention.9,10
Identification of Drivers for Dupilumab PRO Improvements
Dupilumab significantly improved PROs in patients with COPD and Type 2 inflammation in the BOREAS and NOTUS studies; however, the mechanisms underlying this improvement, including QoL and symptom burden, are not well understood.2-4
Causal mediation analysis is a statistical method used to understand the mechanisms through which exposure to a drug affects an outcome by partitioning the total effect of the drug on the outcome into direct and indirect effects based on different mediators. The total effect denotes the overall effect of the treatment on a clinical outcome, while indirect and direct effects estimate the impact with and without mediator(s), respectively.12
To explore the underlying mechanisms by which dupilumab improves PROs, causal mediation analysis was performed on patients with COPD and Type 2 inflammation in the BOREAS and NOTUS clinical trials. The endpoints evaluated were the change from baseline to Week 52 in St George’s Respiratory Questionnaire (SGRQ) and Evaluating Respiratory Symptoms in COPD (E-RS:COPD) total score in the pooled intention-to-treat population. These outcomes measure QoL and symptom burden, respectively. Four key mediators were considered in the analysis: change in the number of moderate or severe exacerbations, change in pre-bronchodilator FEV1, change in post-bronchodilator FEV1, and change in FeNO levels. The analysis was controlled for potential confounding factors, including age, sex, smoking status, region, and the number of moderate or severe exacerbations in the year prior to the study.13
Results of the causal mediation analysis showed that dupilumab’s effect on QoL, as measured by the SGRQ score, was partially mediated by fewer exacerbations, improved lung function, and lower FeNO levels. The total effect of dupilumab versus placebo for change in SGRQ total score was estimated as −3.6, −3.6, −3.5, and −3.6, with change in exacerbation frequency, change in pre- and post-bronchodilator FEV1, and change in FeNO as mediators, respectively.13
Change in exacerbation frequency, change in pre- and post-bronchodilator FEV1, and change in FeNO indirectly affected dupilumab’s total effect on SGRQ by estimates of −0.5, −0.9, −0.8, and −0.5, respectively, mediating 13.3% (95% CI: 3.8–22.8; p=0.006), 25.7% (95% CI: 10.7–40.6; p<0.001), 23.6% (95% CI: 9.4–37.8; p=0.001), and 13.3%(95% CI: 2.5–24.1; p=0.016) of the overallQoL benefit, respectively.13
Similarly, dupilumab’s effect on symptom burden reduction, as measured by the E-RS:COPD, was also found to be partially mediated by reduced exacerbations, improved lung function, and lower FeNO levels. Dupilumab’s total effect on change in E-RS:COPD versus placebo was estimated as −0.9, as mediated by change in exacerbation frequency and change in pre- and post-bronchodilator FEV1, and −0.1, as mediated by change in FeNO.13
Change in exacerbation frequency, change in pre- and post-bronchodilator FEV1, and change in FeNO indirectly affected dupilumab’s total effect on E-RS:COPD by an estimated −0.1–−0.2 points. These mediators were therefore responsible for an estimated 9.8% (95% CI: 0.5–19.1; p=0.039), 24.9%(95% CI: 6.2–43.6; p=0.009), 23.5% (95% CI:5.0–42.0; p=0.013), and 13.6% (95% CI: −0.7–27.8; p=0.062), respectively, of the total dupilumab benefit on symptom burden.13
Overall, results from this causal mediation analysis of the BOREAS and NOTUS studies indicate that PRO improvements with dupilumab in patients with COPD are partially mediated by changes in exacerbation frequency, lung function, and FeNO. Improvement in lung function, in particular, plays a role in QoL and symptom improvement. This supports the interplay between Type 2 inflammatory biomarkers, clinical events, and PROs in patients with COPD treated with dupilumab.13
Phase IV AEOLUS Study of Dupilumab in Airway Remodeling and Mucus Plugging
IL-4 and IL-13, key and central drivers of Type 2 inflammation, contribute to mucus hypersecretion and mucus plug formation via promotion of goblet cell differentiation, excess mucin (MUC5AC) production, and associated mucociliary disruption, leading to poorer disease outcomes in patients with COPD.14-18
The VESTIGE trial showed that dupilumab can reduce mucus plugs and improve small airway function in patients with moderate-to-severe asthma. However, currently, there are limited data on the effect of dupilumab on mucus plugging in patients with COPD.19
Replicating the approach taken in asthma, the multinational AEOLUS study (NCT07053423) has therefore been designed to evaluate the effect of dupilumab on airway resistance and remodeling, including airway inflammation and mucus plugging, in patients with COPD and Type 2 inflammation. Associated improvements in exacerbations, lung function, symptoms, and QoL in dupilumab-treated patients will also be assessed.20
AEOLUS is a Phase IV, randomized, double-blind, placebo-controlled, parallel-group trial that will enroll patients aged 40–85 years with moderate or severe COPD (Figure 2). In total, approximately 218 patients from 23 countries across Asia, Europe, Latin America, and North America will be randomized (2:1) to receive add-on dupilumab (300 mg subcutaneous) or matched placebo every 2 weeks for a total treatment period of 24 weeks. Participating countries include Argentina, Brazil, Canada, China, the EU, Japan, Saudi Arabia, Singapore, South Korea, Switzerland, Taiwan, the United Arab Emirates, the UK, and the USA.20
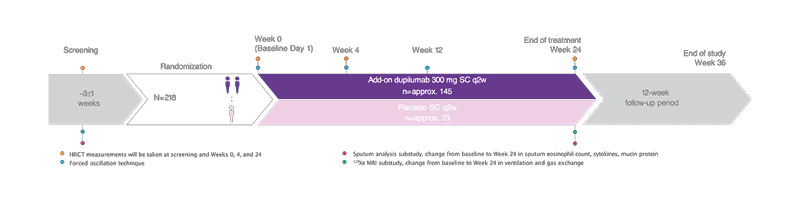
Figure 2: Design of the Phase IV AEOLUS clinical trial.20
AEOLUS will enroll patients (40–85 years) with COPD, moderate-to-severe airflow limitation (post-bronchodilator
FEV1/FVC <0.7 and post-bronchodilator ppFEV1 of 30% to <80%), and Type 2 inflammation (blood eosinophil count ≥300 cells/µL at screening or ≥150 cells/µL at screening with a blood eosinophil count ≥300 cells/µL within the past year).
FVC: forced vital capacity; HRCT: high-resolution CT; ppFEV1: percent predicted forced expiratory volume in 1 second; q2w: every 2 weeks; SC: subcutaneous.
Key patient eligibility criteria for the AEOLUS study are:20
- Former or current smokers
- Physician-diagnosed COPD for ≥1 year with post-bronchodilator FEV1/forced vital capacity ratio ≤0.70 and post-bronchodilator ppFEV1 ≥30% and <80%
- On inhaled triple therapy for ≥3 months before randomization: inhaled corticosteroids, long-acting β2-agonist, and long-acting muscarinic antagonists,or dual therapy if inhaled corticosteroids are contraindicated
- History of high exacerbation risk, defined as ≥2 moderate or ≥1 severe exacerbations in the prior year
- Medical Research Council (MRC) Dyspnea Scale Grade ≥2 or COPD Assessment Test (CAT) score ≥10 at screening
- CT mucus plug score ≥3 at screening
Patients participating in AEOLUS also require evidence of Type 2 inflammation, defined as blood eosinophils ≥300 cells/µL at screening or blood eosinophils ≥150 cells/µL at screening and a history of blood eosinophils ≥300 cells/µL in the previous year. This is slightly more relaxed than the corresponding inclusion criteria for the BOREAS/NOTUS trials, which required blood eosinophil levels to be ≥300 cells/µL at the screening visit.2-4
AEOLUS study exclusion criteria include a prior or current diagnosis of asthma or other significant pulmonary disease; acute exacerbation or respiratory tract infection ≤4 weeks prior to screening; history of clinically significant laboratory findings or abnormal ECG; α-1 anti-trypsin diagnosis; previous use of dupilumab or other biologics/immunosuppressives; controller therapy compliance <80% during screening; recent live attenuated vaccination; oxygen treatment; and treatment with antiarrhythmics, antidiuretics, macrolides, roflumilast, ensifentrine, or mucolytics(unless on a stable dose for >6 months).20
The primary endpoint of the study is the change from baseline to Week 24 in lung mucus score. Scores range from 0–18, with higher scores indicating greater mucus burden and mucus plugging. AEOLUS will also use innovative lung imaging parameters such as high-resolution CT (HRCT), forced oscillation technique, and 129Xe MRI techniques to evaluate key secondary endpoints related to airway remodeling and mucus plugging. These include change from baseline to Week 24 in global mucus volume and trimmed distal airway wall thickness at total lung capacity, measured by HRCT; and the difference in airway resistance from R5 to R20 and reactance area measured by forced oscillation technique. R5 to R20 denotes the difference in airway resistance at 5 Hz and 20 Hz. Treatment-emergent adverse events (TEAE), serious adverse events (SAE), and adverse events of special interest will also be assessed as secondary outcomes, alongside potentially clinically significant abnormalities in hematology, biochemistry, and vital signs.20
AEOLUS will additionally evaluate several exploratory outcomes, including acute exacerbations, lung inflammation (FeNO), oscillometry, healthcare resource utilization, remote monitoring, HRCT imaging, spirometry, PROs, and correlation of mucus score with spirometry and PROs. Substudy analyses will look at the change from baseline to Week 24 in key sputum components: eosinophil counts, cytokines, and mucin protein. 129Xe MRI imaging will also be used to evaluate the change from baseline to Week 24 in ventilation (as measured by ventilation defect percent) and gas exchange.20
As of May 2026, the AEOLUS study was underway and recruiting patients. Study completion is estimated for 2029.21
Long-Term Dupilumab Efficacy Data in Asthma
The efficacy of dupilumab in the treatment of asthma has been demonstrated in multiple clinical trials, including the pivotal Phase III QUEST trial (NCT02414854) and its open-label extension study, TRAVERSE (NCT02134028).22,23 QUEST was a randomized, double-blind, placebo-controlled study in which patients with moderate-to-severe asthma received add-on dupilumab (200 mg or 300 mg) q2w for 52 weeks. In the QUEST study, treatment with dupilumab significantly reduced exacerbation rates and improved lung function, asthma control, and QoL. Safety was consistent with the known dupilumab safety profile.22
TRAVERSE was a large, multicenter, open-label extension study that set out to establish the long-term safety and efficacy of dupilumab over a 3-year period. Patients who received dupilumab in the QUEST trial continued treatment (dupilumab–dupilumab), while those who previously received placebo switched to dupilumab (placebo–dupilumab).23
Impact of Clinical Remission Achievement on Long-TermDupilumab Outcomes
Clinical remission is a recently recognized therapeutic goal in the management of moderate-to-severe asthma.24 In the pivotal QUEST study, 37% of dupilumab-treated patients achieved on-treatment clinical remission at Week 52, where clinical remission was defined as the achievement of four key criteria: 1) no severe exacerbations; 2) no oral corticosteroid use during the study period; 3) stable or improved pre-bronchodilator FEV1 (defined as ≤5% decline from QUEST baseline); and 4) 5-item Asthma Control Questionnaire (ACQ-5) score <1.5. These therapeutic effects were sustained through the TRAVERSE extension study, with more than 70% of patients with Type 2 asthma remaining in clinical remission for up to 2 years.22,25
This post-hoc analysis evaluated whether achieving on-treatment clinical remission in QUEST, as defined above, at Week 52 was associated with sustained clinical benefits through Week 48 of TRAVERSE. It included patients with Type 2 asthma (baselineblood eosinophil count ≥150 cells/μL orFeNO ≥25 ppb) who completed QUEST andenrolled in TRAVERSE. Patients were stratified according to whether they met this composite clinical remission endpoint at Week 52of QUEST.26
The following endpoints were then assessed at Week 48 of TRAVERSE:
- Proportion of patients in remission
- Unadjusted annualized severe asthma exacerbation rates
- Mean change in ACQ-5 score fromQUEST baseline
- Percentage change in pre-bronchodilator FEV1 from QUEST baseline
Baseline demographics and disease characteristics were characterized at QUEST baseline and were broadly similar in patients who achieved clinical remission at Week 52 compared to those who did not. Mean patient age ranged from 46–49 years, and over 50% were female.26
Results from the post-hoc analysis showed that patients who achieved clinical remission at Week 52 of QUEST were more likely to remain in remission at Week 48 of TRAVERSE. In TRAVERSE, 76.9% (placebo–dupilumab) and 74.2% (dupilumab–dupilumab) of patients who achieved remission in QUEST stayed in remission, compared with 44.8% (placebo–dupilumab) and 37.8% (dupilumab–dupilumab) of patients not in remission in QUEST who achieved remission at TRAVERSE Week 48 (Figure 3).26
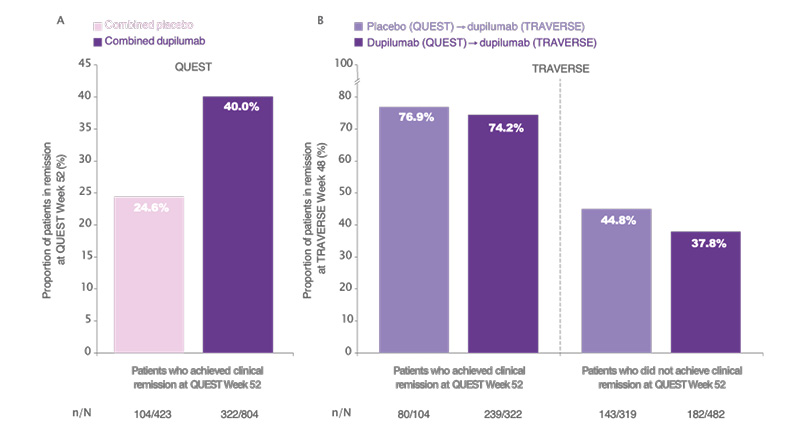
Figure 3: Patients who achieved clinical remission at (A) Week 52 of QUEST were more likely to meet remission criteria at (B) Week 48 of TRAVERSE.26
Exacerbation rates in TRAVERSE were lower among patients who achieved clinical remission in QUEST at Week 52. The unadjusted annualized rate of severe exacerbations was 0.13 (placebo–dupilumab) and 0.10 (dupilumab–dupilumab) in patients who attained clinical remission, compared to 0.41 and 0.43, respectively, in those whodid not.26
Improvements in lung function and ACQ-5 scores during TRAVERSE were also greater in patients who achieved clinical remission in QUEST. Mean increases in pre-bronchodilator FEV₁ from QUEST baseline to TRAVERSE Week 48 were 28.9% (placebo–dupilumab) and 34.1% (dupilumab–dupilumab) in patients who achieved remission in QUEST versus 24.2% and 20.7%, respectively, in patients who did not achieve remission. ACQ-5 scores in TRAVERSE improved by −2.02–−2.09 in patients who attained clinical remission in QUEST, compared to changes of −1.55–−1.58 in those who did not.26
Overall, this post-hoc analysis showed that patients who achieved clinical remission with dupilumab in QUEST were more likely to be in remission and experienced greater sustained clinical effects with long-term dupilumab treatment in TRAVERSE. However, substantial clinical benefits were also observed among patients who did not achieve remission during QUEST.26
These findings support clinical remission as a durable and relevant treatment goal in Type 2 asthma and reinforce the long-term benefits of achieving early disease control with dupilumab.26
Dupilumab in Patients withAsthma and Coexisting Type 2Inflammatory Conditions
The presence of coexisting Type 2 inflammatory conditions can complicate asthma management.27-29 This analysis of the QUEST and TRAVERSE studies therefore set out to evaluate the long-term efficacy of dupilumab in patients with Type 2 asthma and ongoing coexisting allergic rhinitis (n=859), atopic dermatitis (n=142), or chronic rhinosinusitis with nasal polyposis or nasal polyposis (CRSwNP/NP; n=329). Type 2 asthma was defined as baseline blood eosinophil count ≥150 cells/μL or FeNO≥25 ppb. Patients received dupilumab treatment or placebo q2w for 52 weeks in QUEST, followed by dupilumab 300 mg q2win TRAVERSE for up to 96 weeks.30
The study assessments included in this analysis were unadjusted annualized severe exacerbation rates and change from the QUEST baseline in FEV1 and ACQ-5 score over time. These endpoints were analyzed in patients stratified by their coexisting Type 2 inflammatory condition. QUEST baseline demographics, lung function, and disease control were broadly similar for patients in the combined placebo and combined dupilumab groups across the three different Type 2 comorbidities. The mean patient age ranged from 42–52 years, and over 50% were female.30
The results of this analysis showed that dupilumab reduced asthma exacerbations compared to placebo during QUEST, and maintained these reductions through TRAVERSE in patients with ongoing Type 2 coexisting conditions. In QUEST, dupilumab versus placebo reduced exacerbation rates in patients with coexisting allergic rhinitis (0.53 versus 1.10), atopic dermatitis (0.66 versus 1.01), and CRSwNP/NP (0.56 versus 1.52). In TRAVERSE, patients in the placebo–dupilumab group experienced markedly reduced exacerbation rates: 0.33, 0.31, and 0.36 for allergic rhinitis, atopic dermatitis, and CRSwNP/NP, respectively. Patients in the dupilumab–dupilumab group showed further reduced exacerbation rates: 0.32, 0.43, and 0.33, respectively.30
Similarly, dupilumab improved lung function during QUEST and maintained improvements through TRAVERSE in patients with ongoing Type 2 coexisting conditions. Compared to placebo, dupilumab improved pre-bronchodilator FEV1 at Week 52 of QUEST in patients with allergic rhinitis (0.36 versus 0.17), atopic dermatitis (0.41 versus 0.27), and CRSwNP/NP (0.42 versus 0.14). At Week 48 in TRAVERSE, dupilumab treatment improved pre-bronchodilator FEV1 in the placebo–dupilumab group, with changes of 0.38, 0.41, and 0.40 for patients with coexisting allergic rhinitis, atopic dermatitis, and CRSwNP/NP, respectively. Dupilumab also sustained QUEST pre-bronchodilator FEV1 improvements in the dupilumab–dupilumab group: 0.40, 0.42, and 0.43, respectively.30
In patients with ongoing Type 2 coexisting conditions, dupilumab also improved asthma control during QUEST and sustained these improvements during TRAVERSE. Dupilumab reduced ACQ-5 scores compared to placebo by 1.5–1.7 across patients with each of the three different inflammatory comorbidities by Week 52 of QUEST. At Week 48 of TRAVERSE, asthma control improved in both the placebo–dupilumab and dupilumab–dupilumab groups in patients with coexisting allergic rhinitis, atopic dermatitis, and CRSwNP/NP.30
Overall, this analysis demonstrated that dupilumab reduced exacerbation rates and improved lung function and asthma control for up to 2 years in patients with moderate-to-severe Type 2 asthma, despite the presence of coexisting Type 2 inflammatory conditions.30
Itepekimab in COPD: Results from the AERIFY-1 and -2 Trials
Itepekimab is a fully human IgG4 monoclonal antibody that binds with high affinity to IL-33 to block IL-33-mediated signaling. IL-33 is a cytokine triggered by airway insults that has emerged as a potential component in COPD pathogenesis and a promising therapeutic target for treating inflammatory lung disease.31-33 In a previous clinical study, itepekimab was shown to reduce the rate of moderate or severe exacerbations in patients with COPD by 19% and in a pre-specified subgroup of former smokers by 42% (nominally significant).34
The AERIFY-1 and -2 trials were randomized, double-blind, placebo-controlled, international Phase III studies that investigated the efficacy and safety of two doses of itepekimab in former smokers with diagnosed COPD.35 Patients eligible for the study were aged 40–85 years, with moderate-to-severe airflow limitation (post-bronchodilator ppFEV1 30–80%), on stable inhaled triple or dual therapy, and had experienced ≥2 moderate or ≥1 severe exacerbations in the previous year. Patients were required to be former smokers, with cessation ≥6 months before screening.35 A secondary population of current smokers was also included in AERIFY-2 but is not discussed here.35
After a 4-week screening period, patients in both studies were randomized 1:1:1 to itepekimab 300 mg every 4 weeks (q4w), itepekimab 300 mg q2w, or placebo q2w for 52 weeks. In total, 1,127 former smokers with COPD were randomized in AERIFY-1 and 953 in AERIFY-2. The primary endpoint in both studies was annualized rate of moderate or severe exacerbations in former smokers. Change from baseline to Week 24 in pre-bronchodilator FEV1 in former smokers was a key secondary endpoint. Other endpoints included severe exacerbation rate in former smokers and AEs.35
Baseline demographics, disease characteristics, and biomarkers were well-balanced across the treatment arms. The mean patient age was approximately 68 years and the average time since smoking cessation was 9–10 years.35
Looking at the primary endpoint, itepekimab q4w and q2w reduced the rate of moderate or severe exacerbations by 20.5% (p=0.021) and 27.1% (p=0.002) versus placebo in AERIFY-1. The estimated annualized moderate or severe exacerbation rate was 0.71, 0.65, and 0.89 for the three treatment arms, respectively. In AERIFY-2, itepekimab q4w and q2w reduced the rate of moderate or severe exacerbations by 12.4% and 1.6% compared to placebo; however, these differences were not statistically significant. Itepekimab treatment was also associated with numerical reductions in the cumulative mean number of moderate or severe exacerbations in former smokers in the AERIFY-1 and -2 trials.35
In terms of secondary endpoints, itepekimab q4w and q2w significantly reduced the rate of annualized severe exacerbations by 34.1% (nominal p=0.057) and 44.4% (p=0.010) compared to placebo in AERIFY-1. The estimated annualized severe exacerbation rate was 0.09, 0.08, and 0.14 for the two itepekimab arms and placebo, respectively. In AERIFY-2, itepekimab q4w reduced the rate of severe exacerbations by 8.6% compared to placebo, while there was a 7.5% increase compared to placebo in the q2w arm (both p>0.05). In the pooled AERIFY-1 and -2 study populations, the reductions were 21.1% and 22.6% with itepekimab q4w and q2w, respectively, albeit not statistically significant.35
For change in pre-bronchodilator FEV1, itepekimab q4w and q2w demonstrated least squares mean differences versus placebo of 10 mL and 6 mL in AERIFY-1, which were not statistically significant. The corresponding changes in AERIFY-2 were 75 mL and 38 mL, with nominal p-values of <0.001 and 0.031, respectively.35
The safety profile of itepekimab was comparable across both dose groups, and rates of TEAEs, severe TEAEs, treatment-emergent SAEs, and TEAEs leading to discontinuation were broadly similar to placebo. Any TEAEs occurred in 69.5% (n=472) of patients treated with itepekimab q4w, 65.8% (n=460) who received itepekimab q2w, and 66.5% (n=462) on placebo. Rates of treatment-emergent SAEs were 21.5% (n=146), 20.3% (n=142), and 22.2% (n=154), respectively.35
In summary, in former smokers with COPD, itepekimab significantly reduced the rate of moderate or severe exacerbations versus placebo in the AERIFY-1 study but not in AERIFY-2. Similarly, itepekimab showed clinically meaningful reductions in severe exacerbation rates in AERIFY-1, which were not seen in AERIFY-2 or the pooled population. These discordant findings warrant further investigation to evaluate the potential causative. Itepekimab demonstrated an acceptable safety profile across both trials.35
Conclusions
Collectively, these new data presented at ATS 2026 provide further evidence supporting the efficacy profile of the dual IL-4 and IL-13 inhibitor, dupilumab, in treating asthma and COPD in patients with Type 2 inflammation. In particular, post-hoc analyses of pivotal Phase III trials support the potential use of dupilumab earlier in the disease pathway for both COPD and asthma, in order to maximize treatment outcomes. Potential limitations of this evidence include its derivation from post-hoc analyses and the exploratory nature of some findings.






