Abstract
Epilepsy, a chronic neurologic condition, affects nearly 70 million people worldwide, with anti-epileptic drugs as the mainstay of management. Medication adherence is key to successful treatment, reducing seizure frequency, and improving quality of Life (QOL). This study assessed sub-optimum adherence, seizure frequency, QOL, and their socio-demographic and clinical predictors. It was a cross-sectional part of a randomised control intervention on psycho-educational effects at Federal Neuro-Psychiatric Hospital, Maiduguri, Nigeria. A total of 410 adult people with epilepsy (aged 19–65 years) on anti-epileptic drugs for at least 3 months participated. Data analysis using SPSS 18 (IBM, Armonk, New York, USA) showed that 64.9% had sub-optimum adherence, 50.8% were seizure-free in the last 3 months, and 51.7% had good QOL. Independent predictors of poor adherence included being married (odds ratio [OR]: 3.13; p=0.047), having focal seizures (OR: 2.20; p=0.001), and frequent seizure episodes (OR: 4.90; p<0.0001). QOL predictors were age of epilepsy onset (OR: 1.90; p=0.033) and seizure frequency (OR: 2.1; p=0.0001). Non-adherence remains high, yet proper seizure control is achievable, leading to better QOL. Socio-demographic and clinical factors significantly influence adherence and QOL, highlighting the need for psychoeducation in routine care.
Key Points
1. High non-adherence: Nearly two-thirds (64.9%) of people with epilepsy reported sub-optimum adherence to anti-epileptic drugs, highlighting a major barrier to effective management.2. Frequent seizures were strongly associated with poor adherence (odds ratio: 4.90) and worse quality of life (QOL) (odds ratio: 2.1); and better control correlated with better QOL.
3. Marital status (married), focal seizure type, earlier age at epilepsy onset, and higher seizure frequency independently predicted poorer adherence or QOL, supporting targeted routine psychoeducation and tailored clinical follow-up.
BACKGROUND AND AIMS
Epilepsy is one of the common disorders known to man, with early accounts of the disorder traced back to antiquity.1 It was originally thought to be a mystical disease by almost all ancient cultures, such as the Greeks, Egyptians, Babylonians, etc. In modern science, it is defined as the occurrence of at least two unprovoked (reflex) seizures occurring more than 24 hours apart, having one unprovoked (or reflex) seizure and a probability of further seizures similar to the general recurrence risk (at least 60%) after two unprovoked seizures occurring over the next 10 years, or presence of a diagnosis of an epilepsy syndrome,2 and affects nearly 70 million people worldwide.2,3 In high-income countries, seven in 1,000 people will develop epilepsy in their lifetime, while 61 in 100,000 will develop new-onset epilepsy each year.4 These figures are about twice as high in low- and middle-income countries (LMIC).2,3 Problems such as obstetric complications, childhood malnutrition, central nervous system infections, and head injuries are possibly responsible for the high incidence, among other causes. The incidence varies with age, found to be higher in extremes of age and lower among young adults, and higher in LMICs, with 80% of the global burden of epilepsy seen in these countries of the world.2,3
Pharmacotherapy with anti-epileptic drugs (AED) is the mainstay of the management of epilepsy.5 As epilepsy is a chronic condition, patients are usually required to be on long-term treatment with AEDs. Adherence to AEDs, which is the extent to which patients with epilepsy (PWE) follow the mutually agreed recommendations for prescribed medication with healthcare providers,6 is a key determinant of the success of pharmacotherapy among PWE.6-8
Medication non-adherence is generally prevalent among patients with chronic conditions, particularly in LMICs where high out-of-pocket expenditure is prevalent and other socio-cultural and economic factors are influential. In Northeast Nigeria for instance, Wakawa et al.9 reported a 55.7% prevalence of sub-optimal medication adherence among patients with severe mental illnesses. Factors responsible include patronage of traditional and spiritual treatments, male gender, poor insight, and low social support. Similarly, adherence among patients with hypertension in Nigeria is low, ranging from 14–89%, contributing substantially to uncontrolled hypertension and related complications among this population.10
In the context of epilepsy, studies have equally shown that non-adherence to AEDs is prevalent and may be the most important cause of poorly controlled epilepsy.11 Furthermore, Stanaway et al.12 showed that up to 31% of seizures were precipitated by non-adherence to medication. Adherence to AEDs contributes to seizure control and, hence, improved quality of life (QOL).13 Extant literature suggests that sub-optimum adherence is associated with frequent dosing of several medications and drug side effects, age, and poor attitude to taking medication.11,14 Jones et al.15 in the UK, found that 59% of PWE were non-adherent to their AEDs. Ahmad et al.13 found that only 21.2% achieved high levels of adherence. A study in Laos16 showed non-adherence to AEDs to be at 42.4% among PWE. Finally, Mahmoud et al.11 reported up to 80% prevalence of medication non-adherence in Pakistan. Optimum adherence was associated with literacy, being on monotherapy, and less frequent seizures. Similarly, studies by Johnbull et al.17 in Northern Nigeria, and Hasiso and Desse18 in Southern Ethiopia, reported non-adherence rates of 68% and 67.4%, respectively. The most reported reasons for non-adherence were forgetfulness (75.4%) and running out of pills (10.8%). Factors that affected medication adherence were duration of epilepsy treatment, being married, levels of education, absence of comorbidity, forgetfulness, drug-induced fatigue, poor knowledge of AEDs, and being away from home.17,18 In low-resource settings like Northern Nigeria, paucity of healthcare personnel and infrastructure, coupled with inadequate and limited access to AEDs and out-of-pocket purchase of treatment, significantly contribute to non-adherence, leading to poor seizure control, increased morbidity, and a reduced QOL.17
Addressing medication non-adherence among patients with epilepsy requires multifaceted interventions targeting medical, psychological, social, and systemic factors. Both randomised controlled and cohort studies have shown that structured psycho-educational programmes are effective in improving medication adherence and hence treatment outcomes among patients with epilepsy.19-22
The World Health Organization Quality of Life (WHOQOL) group defined QOL as the “individuals’ perception of their position in life in the context of the culture and the value system in which they live and in relation to their goals, expectations, standards, and concerns.”23 It is known that epilepsy has a great negative impact on the QOL of affected patients.24,25 Studies have shown that up to two-thirds of PWE who become seizure-free have a QOL similar to that of the general population.26,27 Medication adherence, polypharmacy, experience of public stigma, low household per capita income, seizure frequency, and severity of seizures are some of the factors that affect the QOL of PWE,28-30 in addition to low self-esteem and self-stigma.31 Other factors that affect QOL include depression, poor occupational adjustment, adjustment to seizure, and seizure worries.32 Suurmeijer et al.33 reported, in decreasing order of importance, that “psychological distress,” “loneliness,” “adjustment and coping,” and “stigma perception” contribute significantly to QOL. Studies have shown that the common predictors of poor QOL among patients on AEDs include anxiety disorders, depressive disorders, frequency of seizures, use of multiple AEDs, female gender, and side effects of AEDs.34,35 The most common aspects of QOL affected according to Imam et al.36 were impaired energy in 46.8% of cases, followed by memory problems (34.4%), fear of experiencing another seizure (25.8%), work (16.7%), and social limitations (10.3%).
There is a paucity of documentation on medication adherence among PWE, especially in sub-Saharan Africa and particularly in northeast Nigeria, where this study was conducted. Poverty and low level of education, which characterise the northeast part of Nigeria, out-of-pocket payment of medical services, and poor knowledge about one’s own disease have been reported to have negative effects on medication adherence.37,38 Epilepsy may likely compound the levels of poverty among its patients, and so does ignorance on the topic, which is prevalent in northern Nigeria. These may affect their level of medication adherence and consequently, QOL.
Based on the available literature searched, most published studies that assessed the relationship between epilepsy and QOL are from developed countries.25,27,28,39 If any such studies were conducted in developing countries, they are sparse and thus not readily accessible. Therefore, there is a need to assess the influence of sociodemographic and clinical factors on medication adherence and the attendant interactions with QOL among PWE in northeast Nigeria.
Aims of this Study
The aims of this study were two prongs: firstly, to assess the prevalence of sub-optimum medication adherence and the level of QOL among PWE in northeast Nigeria, and secondly, to determine the predictors of medication adherence and QOL among the study participants.
METHODS
This study was part of an interventional study on the effect of a psycho-educational intervention on knowledge of epilepsy (KOE), medication adherence, and QOL among PWE on AEDs attending Federal Neuro-Psychiatric Hospital Maiduguri, a tertiary specialist mental health hospital in Borno State, northeast Nigeria. The study was carried out among 410 patients attending the epilepsy clinic of the hospital who participated in the study. Simple random sampling was used to recruit prospective participants who fulfilled inclusion criteria using a table of random numbers from a total of 1,601 PWE who attended the epilepsy clinic during the study period of 16 weeks. Block randomisation and allocation concealment were used to randomise participants into the intervention and the control groups (in the interventional arm of the study). The psychoeducational programme, adapted from the Modular Service Package for the Treatment of Epilepsy (MOSES) by Ried et al.40 and tailored to the local context, comprised four modules covering epilepsy awareness, medical aspects, seizure triggers and avoidance, and lifestyle and treatment adherence. Delivered in group sessions by senior psychiatry registrars, it was conducted over two sessions, each held 4 weeks apart, using a structured, didactic, and interactive approach. The eligibility criteria were patients aged 19–65 years, diagnosed with epilepsy by consultant psychiatrists, having been on follow-up visits and AED treatments for at least 3 months, and who had granted informed consent. Exclusion criteria included patients presenting for the first time and patients with comorbid neuropsychiatric conditions, such as intellectual disability, schizophrenia, dementia, multiple sclerosis, etc.
The Statistical Package for the Social Sciences (SPSS) version 18 (IBM, Armonk, New York, USA) was used to analyse the data collected. Whereas descriptive statistics such as mean, range, and standard deviation were used to describe continuous variables, frequencies and percentages were used to analyse categorical variables. Bivariate analysis using the χ2 test was used to explore associations between sociodemographic variables and clinical variables on one hand, and outcome variables on the other hand. Binary logistic regression was then applied to assess independent predictors of sub-optimum medication adherence and QOL. Sociodemographic and clinical factors were used as covariates, while sub-optimum medication adherence and QOL were independent variables.
Ethical Consideration
Ethical clearance with reference No: FNPHM/REC/2017/05 from the institutional Ethics Review Board of Federal Neuropsychiatric Hospital, Maiduguri, was obtained before conducting the study. Written informed consent forms explaining the study protocol were given to prospective participants, soliciting consent to participate in the study, while assuring them of utmost confidentiality, as only codes instead of names will be employed during data collection and analysis. The research was carried out in accordance with the standard of research involving human subjects as enshrined in the Helsinki Declaration.
Measures
Sociodemographic questionnaire: A pre-designed pro forma questionnaire designed by the authors, soliciting the sociodemographic characteristics of the participants (age, educational status, marital status, tribes, and employment status), was used to collect sociodemographic data.
Clinical variables questionnaire: The clinical pro forma designed by the authors was used to collect the clinical variables, which included the following: seizure type (partial, partial with secondary generalisation, generalised), seizure frequency per month, seizure control for over 3 months (with a response of yes or no), epilepsy duration in years, and types and number of AEDs being used for treatment. Seizure frequency was assessed according to the following four categories: 0: no seizures in the last 3 months; 1: one to three seizures in the past 3 months; 2: four to six seizures in the past 3 months; and 3: more than six seizures in the last 3 months. Those with three or fewer seizures in the past 3 months are defined as having less frequent seizures, while those with four or more seizures have frequent seizures.19,22
Patient case files: Patients’ case files were used to obtain relevant clinical data of the participants, such as the classes of seizures, duration of epilepsy, duration of untreated epilepsy and duration of treatment, numbers and types of medications the patients were taking, and electro-encephalography reports and findings.
Medication Adherence Scale (MAS): The Morisky MAS was used to assess the adherence levels of the participants. It is an eight-item, self-administered scale for medication use attitude and behaviour patterns. Developed by Morisky et al.,41 it involves asking the patients about their drug-taking behaviour patterns and it is validated in sub-Saharan African setting.42 It assesses either the tendency and the extent to which patients forget to take their medication or discontinue it upon feeling better or after their conditions worsens. It also includes the patient’s perception of their treatment plan as either convenient or not.38 Responses are categorised as either ‘Yes’ or ‘No’ for each of the first seven items, with a five-point Likert scale response for the eighth item. Each of the first seven questions is scored as one (1) for a ‘No’ answer and zero (0) for a ‘Yes’ answer. Scores range from 0–8 and are categorised into three adherence levels: a score of 8 indicates high adherence, scores between 5–7 reflect moderate adherence, and scores below 5 denote low adherence. For this study, any score of 7 and below is considered sub-optimum adherence, given the enormity of medication non-adherence in the management of epilepsy. A similar cut-off was adopted by Wakawa et al.9,43 in assessing medication non-adherence among patients with epilepsy and severe mental illness in northeastern Nigeria, as well as by Kretchy et al.44 in assessing non-adherence among outpatients with hypertension and comorbid psychiatric conditions in Ghana. The hospital in which the study was carried out lacks laboratory facilities for serum assessment of drug metabolites for the monitoring of AEDs adherence, which would have been a more objective way of assessing adherence.
Quality of Life in Epilepsy Questionnaire (QOLIE-31): The QOLIE-31 questionnaire is a 31-item, self-administered instrument specifically designed to measure the QOL of PWE. It was derived from QOLIE-89.45,46 The QOLIE-31 questionnaire consists of seven of the 17 subscales of QOLIE-89. The QOLIE-31 questionnaire has two subscales: the emotional or psychological effects subscale (seizure worry, overall QOL, emotional wellbeing, energy, or fatigue subscales) and the medical and social effects (medication effects, work-driving social limits, cognitive function) subscale. It is scored from 0–100. Responses are summed up to give rise to the subtotal of the subscale scores and the overall total score. Higher scores on the QOLIE-31 indicate better levels of functioning and QOL. The QOLIE-31 has good psychometric properties, with Cronbach’s alpha internal consistency of 0.85, and a test-retest reliability of (r=0.85).45 Ogundare et al.47 used it in Nigeria. It takes approximately 10 minutes for an individual with normal intelligence to complete it.45 Based on this study, those who scored below the mean score of 50.1 were categorised as having poor QOL and those who scored above the mean were considered to have good QOL. The selection of 50.1, the mean QOL score of the participants, was necessitated by the inability of the authors to access published data on the local average QOLIE-31 score in the study setting. Moreover, the use of a mean score to dichotomise outcome variables aligns with the approach adopted in previous studies, such as Wakawa et al.9 in Nigeria and Kretchy et al.44 in Ghana.
RESULTS
Sociodemographic Characteristics of the Participants
The study participants comprised 230 males (56.1%) and 180 females (43.9%), for a total of 410. The participants’ ages ranged from 19–64 years, with a mean age of 31.6 years and a standard deviation (SD) of ±9.5. The Kanuri tribe was the main ethnicity of the participants, accounting for about half of the study population (193; 47.1%). This is followed distantly by the Hausa tribe (65; 15.9%), then Babur (33; 8.0%), Fulani (31; 7.6%), and other tribes (88; 21.5%). One hundred and sixty-eight (41.0%) of the participants had only Qur’anic education, 113 (27.6%) had high levels of educational attainment (i.e., having ≥12 years of formal education), and the remaining participants had either no education at all (34; 8.3%), or low levels of education (≤11 years of education; 95; 23.2%). Furthermore, approximately half of the participants (187; 45.6%) were unemployed, and 188 (45.9%) were single. Other findings on the sociodemographic characteristics are presented in Table 1.
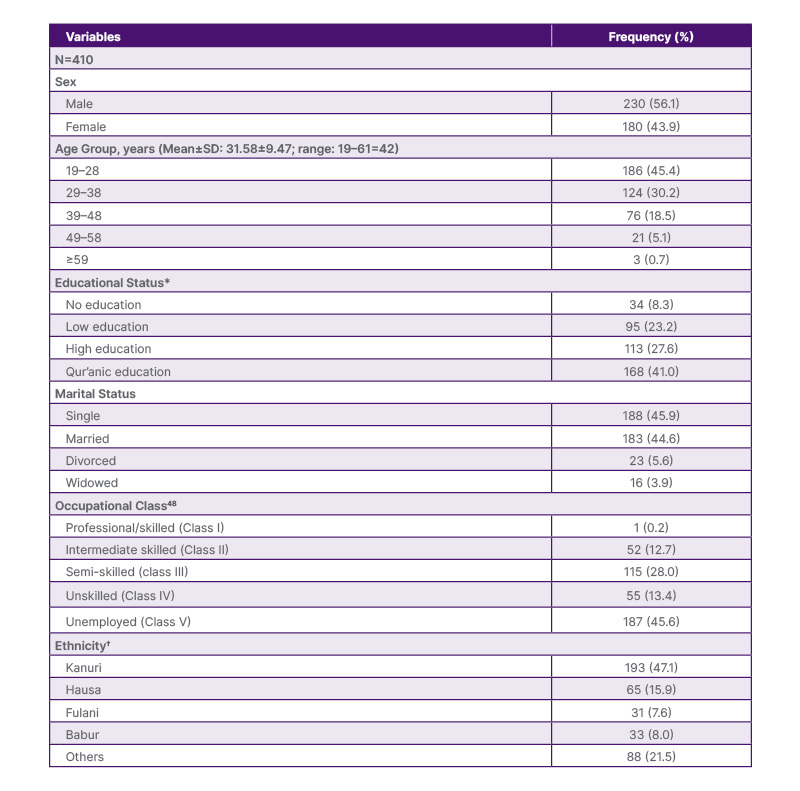
Table 1: Sociodemographic characteristics of the participants.
*High education is having ≥12 years of western education. Low education is <12 years. †Other major ethnicity assessed included Yoruba, Igbo, Marghi, Bolewa, and Shuwa.
Clinical Characteristics of the Participants
A total of 223 (54.4%) had focal seizures, whilst 187 (45.6%) had generalised seizures. About 50.0% of study subjects had no seizures in the last 3 months prior to the study. Participants on single drug therapy constituted the vast majority of participants (383; 93.4%), and only 27 (6.6%) were on polytherapy. The mean age of onset and duration of epilepsy in years were 19.12±1.15 (Mean±SD; range: 0–59=59) and 12.32±9.12 (range: 0.5–42=41.50), respectively. The mean duration of untreated seizure in years was 5.23±5.8 (range: 0–32=32), while the mean seizure frequency in the last 3 months was (Mean±SD) (2.46±3.21) (range: 0-14=14). Other clinical characteristics of the participants are presented in Table 2.
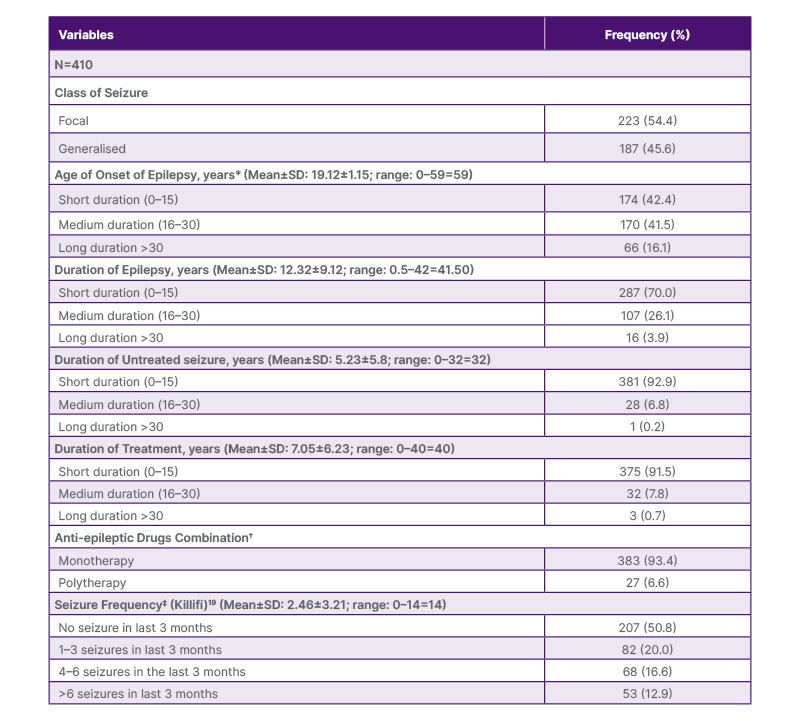
Table 2: Clinical characteristics of the participants.
*0–15 is a short duration of epilepsy, 16–30 is a medium duration, and >31 is long duration.
†Majority of the patients were on carbamazepine, polytherapy constituted mostly of a combination of two drugs (commonly, carbamazepine and sodium valproate or carbamazepine and phenobarbitone).
‡Seizure frequency categories adopted from Ibinda et al.17 Those with three or fewer seizures in the last 3 months are defined as having less frequent seizures, while those with four or more seizures have frequent seizures.
Prevalence/Levels of Medication Adherence and Quality of Life
The majority of the study participants (266; 64.9%) had poor medication adherence, and only about half of the participants (212; 51.7%) had good QOL. Furthermore, about 50% of the participants had at least one seizure episode in the last 3 months. Other findings are represented in Supplementary Table 1.
Association Between Sociodemographic Characteristics and Medication Adherence
Except for marital status (p=0.031), there were no significant relationships between the participants’ sociodemographic characteristics and levels of medication adherence. Other findings on the relationship between sociodemographic characteristics and medication adherence are presented in Supplementary Table 2.
Association Between the Sociodemographic Characteristics and Quality of Life
There was no significant relationship between the sociodemographic
Association Between Clinical Variables and Medication Adherence
The combination of classes of seizures (p<0.0001), seizure frequency (p<0.0001), and AEDs (p=0.022) had a significant relationship with medication adherence. Other findings are represented in Supplementary Table 3.
Association Between Clinical Variables and Quality of Life
Among the clinical variables assessed, seizure frequency (p<0.0001) and age of onset of epilepsy (p=0.044) had significant relationships with levels of QOL. Other findings are represented in Supplementary Table 4.
Independent Predictors of Medication Adherence and Quality of Life
Class of seizures (p=0.001), seizure frequency (p<0.0001), being married (p=0.047), and AEDs combination (p=0.047) were independent predictors of medication adherence. The age of onset of seizure (p=0.044) and seizure frequency (p<0.0001) had a statistically significant relationship with QOL at bivariate analysis. These same variables were independent predictors of QOL. These findings are depicted in Table 3.
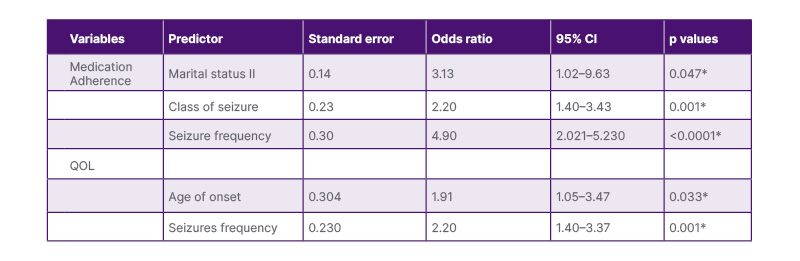
Table 3: Independent predictors of seizure frequency.
*Statistically significant. QOL: quality of life.
DISCUSSION
Fifty-six percent of the participants were males with a mean age of 31.6 years (±9.5), 41.0% of the participants had only Qur’anic education, 27.6% had high levels of educational attainment (i.e., having ≥12 years of formal education), and the remaining participants had either no education at all (8.3%), or low levels of education (≤11 years of education; 23.2%). Furthermore, approximately half of the participants were unemployed (45.6%) and single (45.9%). Focal seizures were recorded in 54.4% of the participants, while 45.6% had generalised seizures and 50.8% had no seizures in the last 3 months before the study. About 65% (64.9%) had sub-optimum medication adherence, and 51.7% had good QOL. The independent predictors of sub-optimum medication adherence were being married, having focal seizures, and frequent seizure episodes, which were more likely to be less adherent to medication than those with lower seizure frequency. The independent predictors of QOL include the age of onset of epilepsy and seizure frequency.
Sub-optimum Medication Adherence
The finding of more than half (64.9%) of the participants in this study having poor medication adherence is in keeping with many previous studies. For example, Ahmad et al.13 reported medication non-adherence of 78.8%. Similarly, Hasiso and Desse18 in Ethiopia found non-adherence of 68%. Although the most common reasons for the non-adherence in the Ethiopian study were forgetfulness (75.4%) and running out of pills (10.8%), other factors such as poverty, out-of-pocket purchase of AEDs,49 medication side effects, attitudes to medications, and poor KOE and AEDs may, generally, account for the low levels of adherence found in this study. Furthermore, Johnbull et al.17 in northern Nigeria, and Jones et al.14 in the UK, found 67.4% and 59.0% of PWE were non-adherent to their treatments, respectively. Other concordant findings include studies from Brazil, Nigeria, and Palestine, where they showed non-adherence rates of 66.2%, 67.4%, and 64%, respectively.2,50-52 One strong basis for comparison among these studies is the use of the Morisky MAS.
On the contrary, Gurumurthy et al.51 and a study from Laos showed adherence was found to be 72.3% and 57.6%, respectively, among PWE.16 These two studies were consistent with the studies in the UK (63.6%) and the USA (73%).2,53 The variation in non-adherence rates across studies may be attributable to differences in study designs, as well as the sociodemographic and clinical characteristics of participants. Factors such as socio-cultural attitudes, educational and economic status, and the extent of social or health insurance coverage may also contribute to these disparities.51 Poor KOE, low level of education, unemployment, out-of-pocket payment of medication, and other sociodemographic factors could be responsible for the poor adherence.
Sociodemographic Predictors of Sub-optimum Medication Adherence
Participants who were married were three times less likely to be adherent to AEDs, followed by those who were divorced. This result is rather unexpected, as spouses of chronically ill patients could likely serve as treatment helpers, reminding them to take their medication since forgetfulness is a factor for poor adherence.17 The possible explanation for this result could be that married participants might be shouldering more responsibilities, financial and others, which may distract them from being adherent. Additionally, non-adherence among married participants may be a result of the sexual side effects of the AEDs.54 This finding is in contrast to that of Hasiso and Desse18 in Southern Ethiopia. The index study did not find, however, any significant association between medication adherence and other sociodemographic variables. Gurumurthy et al.51 similarly reported no significant association between age, gender, and medication adherence. Gurumurthy et al.51 and Das et al.,55 both in India, reported a significant relationship between AED adherence and socioeconomic class. This is not in keeping with the findings of this study; differences in sociodemographic characteristics of the participants of the various study settings and the study designs might account for this contrast. Johnbull et al.17 reported similar findings: apart from knowledge of AEDs, there was no significant association between age, sex, educational status, marital status and income or occupational status, and medication adherence.2 In low-resource settings like northern Nigeria, paucity of healthcare infrastructure and personnel and inadequate and limited access to AEDs, coupled with out-of-pocket purchase of treatment, significantly contribute to non-adherence, leading to poor seizure control, increased morbidity, and a reduced QOL.17
Clinical Predictors of Sub-optimum Medication Adherence
Class of epilepsy (p<0.0001), seizure frequency (p<0.0001), and AEDs combination (p=0.022) were associated with medication adherence. Participants with focal, less frequent seizures and those on monotherapy were more likely to be adherent to AEDs than those with frequent seizures and those on polytherapy. Multivariate binary logistic regression revealed that all three variables were found to be independent predictors of medication adherence. Participants with focal seizures were about twice as likely (odds ratio [OR]: 2.20; p=0.001; 95% CI: 1.38–3.43) to be non-adherent to medication than those with generalised seizures. Participants with frequent seizure episodes were five times (OR: 4.90; p<0.0001; 95% CI: 2.02–5.23) more likely to be non-adherent to medication than those with infrequent seizure episodes. Participants on monotherapy were about three times (OR: 3.31; p=0.030; 95% CI: 1.12–9.77) more likely to be adherent to medication than those on polytherapy. The probable explanation for this finding could be that the cost of buying more than one medication and taking more than one drug with multiple-dose regimens may reduce the chances of adherence among the participants. Other clinical variables assessed were not associated with medication adherence. The work of Gabr and Shams56 supports these findings. In addition, Gabr and Shams,56 Bautista and Rundle-Gonzalez,57 and Harimanana et al.16 revealed that monotherapy is more associated with optimum adherence than polytherapy. Higher pill burden and occurrence of side effects, multiple daily dosing schedules, and higher cost of the AEDs were postulated to be the possible reasons. However, Gurumurthy et al.51 showed no significant association between seizure frequency and adherence. Furthermore, Gurumurthy et al.,51 as well as Sweileh et al.,58 showed no significant association between levels of adherence and AEDs combination.2
Duration of epilepsy treatment is likely to have a negative relationship with medication adherence, due to the long duration of pill burden and cost of medication, among other factors, as supported by Hasiso and Desse’s18 study in Southern Ethiopia. Gurumurthy et al.,51 Mbuba et al.,59 El-Shamaa et al.,60 and Kyngäs,61 who all reported that medication adherence was associated with duration of epilepsy treatment and absence or presence of comorbidity, which is contrary to the index study. However, the findings of this study, as well as those of Gurumurthy et al.51 and Gabr and Shams,56 did not support this.
Level of Quality of Life
It is observed that epilepsy significantly impacts negatively on the QOL of the patients.34,62 The concept of QOL in epilepsy encompasses physical health, mental health, and social health.34 Numerous factors contribute to the low level of QOL seen among PWE. Slightly more than half (51.7%) of the participants had good QOL. This finding may be connected with the fact that about 50.5% of the participants had no seizure episode in the past 3 months before the study. Numerous studies, particularly in Nigeria, have illustrated that there is an inverse relationship between seizure frequency and QOL.37,62 Another possible reason could be that the perception and idea of the concept of QOL may not be well established among the participants, considering their level of education and awareness, and other sociodemographic peculiarities. Social desirability while responding to the questionnaires could also contribute to this finding.
Ranjana et al.63 found a similar pattern they reported the mean QOL (mean±SD) as 64.1±15.97 among their study participants with individual scores ranging from 15.97–100, although they used QOLIE-10, which is an abridged version of the QOLIE-31 used in this study. Gholami et al.,64 however, reported different patterns in which more than 50% of their study participants had a moderate to low QOL, in contrast to more than 50% of healthy controls, who had good to excellent QOL. This finding is supported by the systematic review study of Baranowski.65 Their study is also consistent with many other previous studies carried out across different countries and cultures: Shakir,66 Tunisian,67 and Stavem et al.68 studies compared QOL of PWE to healthy persons.
Sociodemographic Predictors of Quality of Life
None of the sociodemographic characteristics assessed were found to have an association with QOL. This finding is supported by the work of Phabphal et al.69 in Thailand, although the female gender reported by Mosaku et al.37 in Nigeria and poor occupational adjustment reported by Devinsky and Cramer32 contribute significantly to poor QOL. This could be a negative association, as females are more likely to be poor in Africa, while poor occupational adjustment has an indirect relationship with economic capabilities, which are determinants of QOL. This suggests that clinical factors rather than sociodemographic parameters have more influence on QOL among PWE. Shakir and Al-Asadi,66 however, reported that older patients and those with low education and income levels had lower overall QOL scores.66,69,70
Clinical Predictors of QOL in terms of clinical variables, the age of onset of epilepsy (p<0.0001), and seizure frequency (p<0.0001) were associated with QOL among the participants. Those with the age of onset after the age of 30 years had better QOL than the remaining participants. This means that the shorter the duration patients live with the disease, the better the QOL. Likewise, participants with less seizure frequency had better QOL. These clinical variables (age of onset and seizure frequency) were still found on multivariate logistic regression to predict QOL and for the age of onset (OR: 1.913; 95% CI: 1.054–3.474; p=0.033) and seizure frequency (OR: 2.170; 95% CI: 1.397–3.372; p=0.001). Participants with an earlier age of onset were twice as likely to have poor QOL as those with late ages of onset. Likewise, participants with frequent seizure episodes were about twice as likely to have poor QOL as those with less frequent seizures. Adewuya and Oseni,62 Mosaku et al.37 in Nigeria, Phabphal et al.69 in Thailand, Molugulu et al.71 in India, and Shakir and Al-Asadi66 in Iraq, similarly, revealed that the frequency of seizures predicts poor QOL in PWE.34 Additionally, Mosaku et al.37 found that polytherapy was associated with poor QOL among PWE. Shakir and Al-Asadi66 and Guekht et al.39 also showed duration of epilepsy was significantly associated with QOL scores: the longer the duration, the poorer the QOL. On the other hand, Devinsky and Cramer32 and Suurmeijer et al.33 in the Netherlands showed that the frequency of seizures did not contribute significantly to QOL among PWE, and Suurmeijer et al.33 showed that even the age of onset of epilepsy did not relate to QOL. Furthermore, Suurmeijer et al.33 showed that none of the clinical variables (age at onset, seizure frequency, side effects of AEDs) was predictive of QOL.
LIMITATIONS
This study is not without some limitations. The following were observed to be the limitations of the study:
- The lack of facility for serum assessment of drug metabolites for monitoring of adherence to AEDs, which would have been more objective measures of adherence to medication than the use of Morisky MAS.
- Although using a seizure logbook by PWE for the monitoring of seizure frequency is not common practice in the study setting, the use of logbooks could have added to the objectivity for the reporting of seizure frequencies by the participants, since verbal reporting is more subject to forgetting.
- Because it is a hospital-based and unicentric study, the findings may not be generalised to other settings.
- There was low representation of the populations from other parts of the Northeast geopolitical zone of Nigeria, the catchment area of the study centre, as a result of the security challenges occasioned by the Boko Haram insurgency.
RECOMMENDATION FOR FUTURE DIRECTIONS
Based on the findings of the study, the following recommendations are therefore made:
- The need to incorporate psychoeducation and adherence counselling sessions for PWE as part of the routine clinical services provided for this set of patients.
- The need to conduct a similar study on a larger scale, involving multiple centres across a wider part of the nation.
- The need to have facilities for laboratory serum monitoring of AED levels for clinical and research utilities.
- The need for a study to deeply assess factors that contribute to the high levels of sub-optimum medication adherence observed in the study, and to address them.
CONCLUSION
Based on the outcomes of the study, the following can be inferred: that non-adherence is high among PWE; however, seizure control can be achieved in a significant proportion of PWE, and a good percentage of patients can have fair QOL. Sociodemographic and clinical factors have significant relationships with and can be independent predictors of medication adherence and QOL.






