BACKGROUND AND AIMS
Pregnancy has been considered an immunological paradox due to the need for a perfect balance between immune surveillance/defense to avoid infection of the maternal-fetal interface, and immune tolerance to the fetus to prevent early rejection of the semi-allogenic product.1 It has been shown that, if this balance leans towards one of these ends, preterm birth (PTB) can occur, which is a leading cause for infant mortality and disability worldwide.2 For instance, pioneering studies show that the rate of positive amniotic fluid cultures is 21.6% in PTB cases,3 but increases to 75% when preterm pre-labour rupture of membranes occurs.4 On the other hand, enhanced local T helper 1-type inflammation, either sterile or infection-related, has also been found to strongly associate with PTB.5
In this context, a four-step ascending process for microbial infections has been proposed, where an alteration of the vaginal microbiota is the first step for chorioamnionitis.6 This way, eubiotic microbiota is thought to protect from both infection and inflammation,7 an idea that has been cemented through recent research that shows enhanced humoral and innate inflammation in Lactobacillus spp depleted patients, and that such changes are associated with PTB.8 Nonetheless, the immunologic mechanisms associated with both eubiotic and dysbiotic states are only beginning to be understood, and the authors believe that further studies investigating the microbiome-derived effects on the immune response are needed to fully comprehend this phenomenon.
Thus, in the present study, the authors aimed to describe the community state type (CST)-associated immunosecretomes in order to understand the protective mechanisms of eubiotic microbiota (CST Types I, II, III, and V) and the pathophysiological immune mediators that are produced in dysbiotic (CST IV) subjects.
MATERIALS AND METHODS
A Luminex® immunoassay (Diasorin, Saluggia [Vercelli], Italy) was used to quantify cytokines in the cervico-vaginal samples of 133 subjects at risk of PTB, whereas 16S ribosomal RNA sequencing was used to classify the samples into the CSTs.8 The authors next studied the cytokine-secretion patterns from the cervico-vaginal samples by means of a principal component (PC) analysis for each CST. Moreover, the authors studied the correlation of such PCs with PTB by calculating the odds ratios (OR). Finally, the authors characterised the immunosecretomes of all the subjects who presented PTB, disregarding theirCST status.
RESULTS
In the CST IV patients, the authors found only one of three PCs that correlated with PTB (OR: 18.53; 95% CI: 2.8–202; p=0.0008) that was composed of high levels of IL-5, TNF-α, granulocyte-macrophage colony-stimulating factor (GM-CSF), IL-1β, IL-4, IL-8, interferon-γ (IFN-γ), and IL-10, but low IL-2, IL-6, and IL-18. No other CST-related PC was associated with PTB. Interestingly, the same PC was found when all patients presenting PTB were studied, and 73% of such subjects presented an eubiotic vaginal microbiome (32% CST I, 12% CST II, and 29% CST III), while only 27% belonged to the CST IV class. The other two PTB-associated PCs were rich in IL-4, IL-8, IL-10, IL-2, IL-5, and GM-CSF (for PC2), or IFN-γ, IL-2, IL-5, and TNF-α (for PC3). These two immunosecretomes are also associated with varied CSTs (43% CST I, 26% CST II, 22% CST III, and 9% CST IV for the PC2, and 89% CST I and 11% CST V for the PC3; Figure 1).
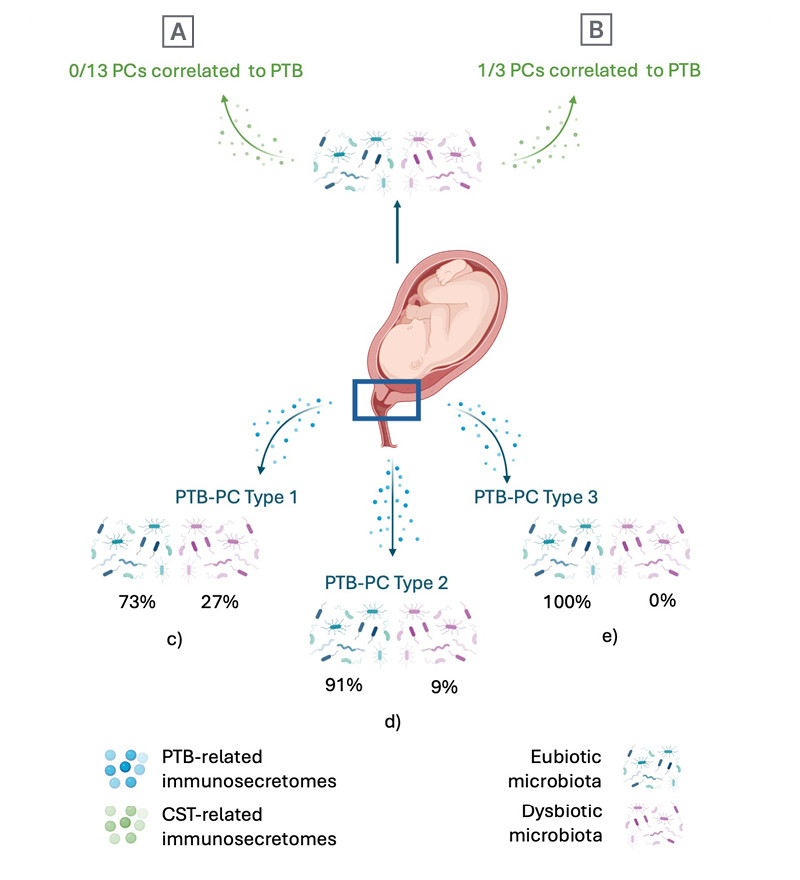
Figure 1: Pre-term birth correlates with distinctive inflammatory profiles, independent of the cervico-vaginal microbiota.
When PCs were studied in subjects with different CST: A) 13 PCs were found in eubiotic subjects, but neither one
correlated to PTB; whereas B) only one of the three PCs found in dysbiotic subjects correlated to PTB. When PCs were studied in patients who presented with PTB, three distinct immune-secretion patterns were found: C) the first one was found to be mostly related (73%) to eubiotic microbiota; D) as well as the second (91%); and E) the third was only found in relation eubiotic states (100%).
CST: community state type; PC: principal component; PTB: preterm birth.
Finally, a PC-regression showed that only IFN-γ, IL-10, TNF-α, GM-CSF, IL-18, and IL-6 are significantly associated with PTB.
CONCLUSION
These results suggest that the aforementioned immunosecretomes, rather than CST status, enhance the risk for PTB. Moreover, the immune response during pregnancy, and therefore the PC status, does not appear to be CST determined. Other factors may be involved in the regulation of inflammation during pregnancy, and further research is needed to understand both the origin and the clinical implications of such findings.