BACKGROUND AND AIMS
Many early antimicrobial stewardship (AMS) initiatives focused on reducing antimicrobial use (AMU). However, reducing AMU may cause harm. To avoid unintended consequences, the focus is now moving to increasing appropriateness of AMU. At the same time, there has been a shift from a single-context approach towards a unified, One Health AMS approach. However, the lack of an agreed definition of appropriate AMU between stakeholders representing animal, human, and environmental health remains a barrier to coordinated, One Health AMS implementation.
METHODS
The authors conducted a literature review and held four focus groups with diverse stakeholders to develop a list of proposed statements that could describe appropriate (systemic) AMU across all One Health contexts.1 The authors included these in a four-round, online Delphi survey circulated to AMS experts globally, whom the authors identified from their publications, professional networks, project partner organisations, and snowballing. Each statement was rated on a seven-point Likert scale (0–6); a score of four or more was considered agreement. Participants could also provide written feedback on each statement. Statements were included in the consensus only when they reached 80% agreement. Those with <60% agreement in any round were considered rejected, and statements with 60–80% agreement were presented again in the subsequent round, until round three, with changes based on participant feedback. In the fourth round, the authors asked the feasibility of measuring each consensus item in the context with which the participant was most familiar.
RESULTS
The authors invited 391 AMS experts to participate, and 243 from 44 countries (62%) provided a response to at least one survey round. Twenty-two percent were from low- and middle-income countries, and 63% were in a position to influence their national AMR strategy. Sixty-three percent represented human health, 26% represented animal health, and 11% environmental health or ‘other’. In round one, 43 of 76 proposed statements (Table 1) reached 80% consensus, with a further eight statements reaching consensus over subsequent rounds. Consensus statements covered a wide range of topics, including who should receive systemic antimicrobials; when, why, and how these should be initiated; and whether it should be for a therapeutic or preventative indication. The selection of drug, route, dosing, and duration were the other main topics; in general, participants agreed that relevant guidelines should be followed, where these are available. In the absence of guidelines, participants agreed that the narrowest spectrum or lowest importance drug should be used, by the safest effective route, and for the shortest duration to control the infection (or risk of infection, in the case of preventative use). The median proportion of respondents who felt that, in their context, it would be feasible to measure concordance with each statement was 62%, with feasibility almost always rated higher for human health contexts than animal health contexts. Statements that were rejected in the first round included: using antimicrobials for the purpose of growth promotion in livestock and using preventative antimicrobials for the purpose of avoiding economic loss.
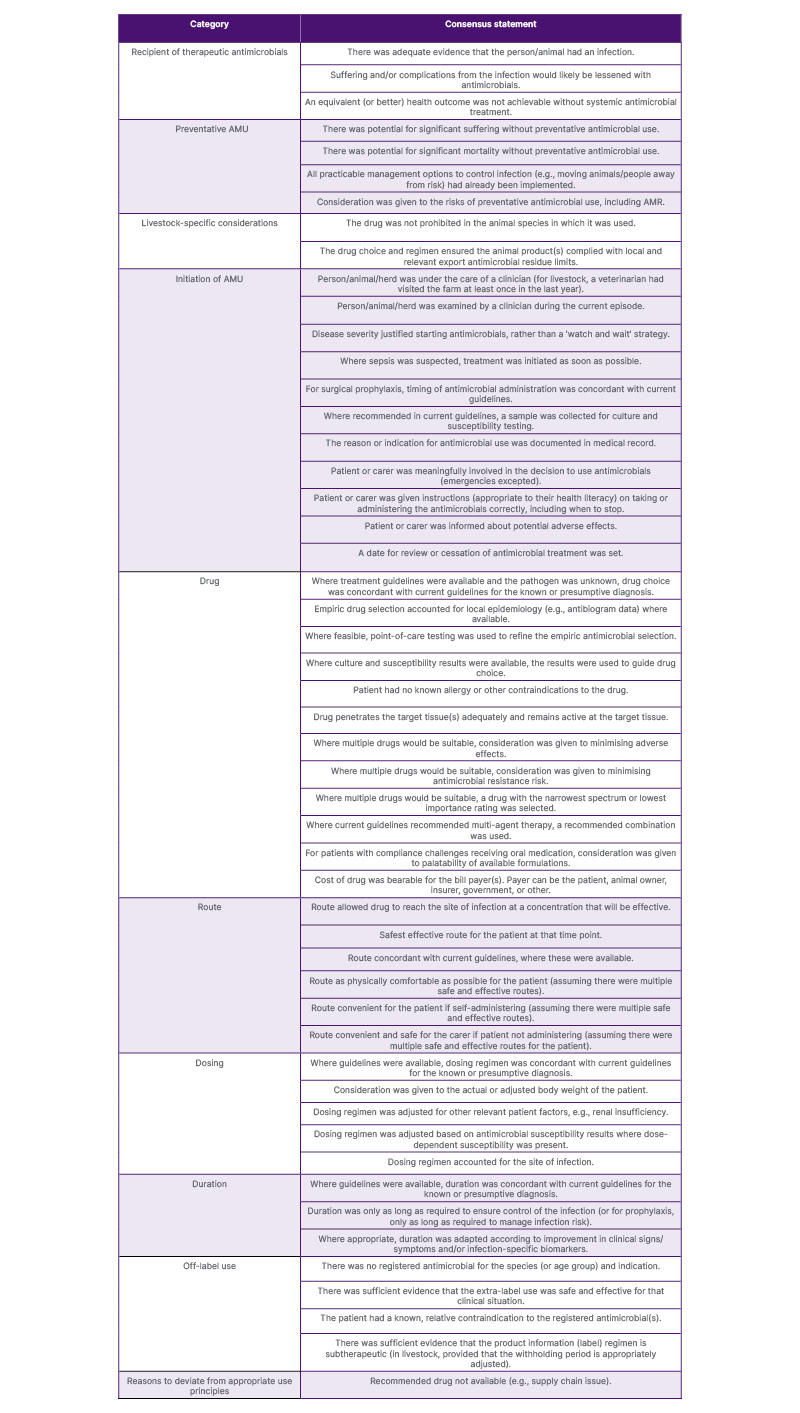
Table 1: The 51 consensus statements regarding important features of appropriate AMU, with the survey question: when considering whether a systemic use of antimicrobials was appropriate, how important is the following?
AMR: antimicrobial resistance; AMU: antimicrobial use.
CONCLUSION
The 51 consensus items from this global survey form a new foundation for further One Health discussion around appropriate AMU and unified measures of appropriate use.




