BACKGROUND AND AIMS
Vestibular migraine (VM) is a common migraine subtype characterized by recurrent vestibular symptoms. Despite its prevalence, evidence-based treatment guidelines are lacking.1-4 Vestibular rehabilitation (VR) has been proven effective in many vestibular disorders, but its role in managing VM has not been well established.5 This systematic review aimed to summarize and pool the evidence on the effectiveness of VR for VM using standardized outcome measures, primarily focusing on patient reported dizziness-related quality-of-life assessments.
MATERIALS AND METHODS
The authors systematically searched MEDLINE, Embase, Cochrane Library, and Scopus from inception to March 2025. Studies were eligible if they enrolled adults with vestibular migraine diagnosed using recognized criteria and reported at least one relevant clinical outcome after a clearly described VR intervention. Meta-analysis of mean change in Dizziness Handicap Inventory (DHI) scores was performed. Risk of bias was assessed using the Cochrane RoB 2 tool for RCTs and the ROBINS-I tool for observational studies.
RESULTS
Seven studies comprising 413 patients (mean age: 45.4; 76% female) with VM treated with VR were included. The effect of vestibular rehabilitation on DHI scores showed a pooled mean difference of −29.3 (95% CI: −40.2–−18.3), more than the clinically important difference of 18 points (Figure 1). However, the authors’ meta-analysis had high heterogeneity.
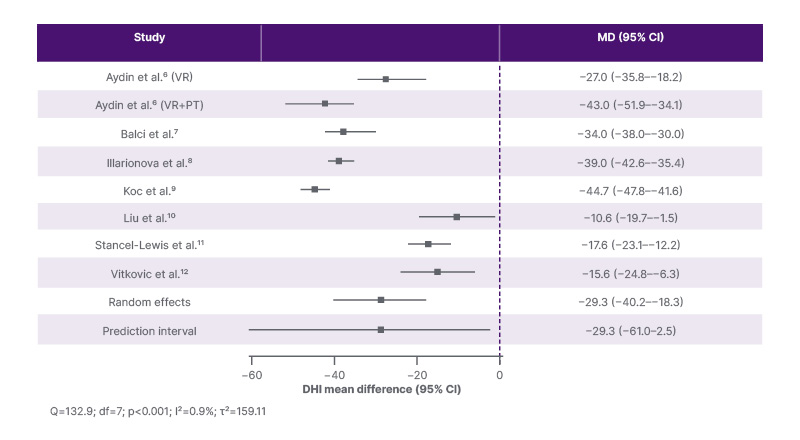
Figure 1: Forest plot of change in DHI scores using a 0.5 correlation assumption.
DHI: Dizziness Handicap Inventory; MD: mean difference; VR: vestibular rehabilitation.
Across studies, the most commonly used rehabilitation elements were habituation exercises, adaptation training, gaze stabilization, balance training, and gait training. Programs ranged from 4 weeks to about 30 weeks, and some were supervised in clinic whereas others relied largely on home exercise programs with remote follow-up.
This variability is clinically relevant because vestibular rehabilitation is often discussed as a single intervention when, in practice, it encompasses multiple distinct treatment strategies.
CONCLUSION
VR demonstrated a reduction in DHI scores, meeting the clinically significant difference of 18, indicating clinical improvement.13 However, the considerable heterogeneity limits the generalizability of these results. Despite these limitations, the authors’ findings support VR as a promising nonpharmacologic option for vestibular migraine, particularly for reducing dizziness-related disability, while also underscoring the need for better-designed randomized studies. Future trials should standardize diagnostic criteria, define VR protocols more clearly, account for concomitant preventive therapy, incorporate objective balance measures, and evaluate durability of response over longer follow-up.






