Abstract
Background: Human papillomavirus (HPV)-associated cancers, such as cervical cancer, are more prevalent in kidney transplant recipients (KTR). Historical data, prior to an established national screening programme, suggest cervical screening uptake in KTRs is low. Little is known about HPV vaccination uptake in KTRs in Ireland. This study aimed to investigate cervical screening and HPV vaccination uptake in KTRs, while identifying patient-level barriers to the same.
Methods: A retrospective cohort study was conducted in two groups in a single centre: firstly, all female KTRs ≤65 years regarding cervical screening, and secondly, all KTRs ≤45 years regarding HPV vaccination status. Telephone questionnaires were administered to patients who consented.
Results: Regarding cervical screening, 42 of 217 eligible female KTRs ≤65 years consented to participate, with three then excluded due to prior hysterectomy. The mean age was 45.3 years (SD: 10) and the mean transplant vintage was 123.6 months (SD: 86.2). Thirty-four patients (87%) had undergone screening since transplantation, and all of those reported adherence with annual screening. Of the five patients (13%) who had not had screening, two indicated this was due to no communication from the screening programme. Awareness of a specific recommendation for annual cervical screening in KTRs was present in 27 patients (69%). Abnormal cervical screening had occurred in 18 patients (46%).
Regarding HPV vaccination, 23 of 48 eligible KTRs who were ≤45 years consented to participate. The mean age of this cohort was 37 years (SD: 6.1) and the mean transplant vintage was 86.3 months (SD: 60.4). Five patients (22%) were HPV vaccinated. There was awareness that KTRs have an increased cancer risk in 20 patients (87%), but only 9% and 4% were aware that HPV vaccination could reduce cancer risk and is Health Service Executive (HSE) guideline recommended, respectively. For unvaccinated KTRs (n=18), all patients stated that they would accept HPV vaccination if provided at their hospital without charge.
Conclusion: Engagement with cervical screening in this cohort of KTRs was high. A risk of self-selection bias exists and a larger, nationwide study is warranted. Low awareness exists on the recommendation and importance of HPV vaccination for KTRs. Unvaccinated patients were highly willing to receive HPV vaccination if administered at their transplant centre.
Key Points
1. Kidney transplant recipients are at a higher risk of human papillomavirus (HPV)-related cancers than the general population. There is a historical low uptake of both cervical screening and HPV vaccination in this cohort.2. The authors conducted two surveys of kidney transplant recipients to identify current adherence with cervical screening recommendations and the prevalence rate of HPV vaccination in an Irish cohort.
3. Cervical screening adherence was higher than previously reported, but a risk of bias exists. HPV vaccination rates were low. While many kidney transplant recipients were aware of their increased cancer risk, they were mostly unaware of the potential benefits of HPV vaccination in reducing cancer risk and that HPV vaccination is guideline recommended.
INTRODUCTION
Kidney transplant recipients (KTR) face a higher risk of developing cancer than the general population due to immunosuppression therapy.1 Cervical cancer is the fourth most common cancer in women worldwide, accounting for 6% of all female cancers, but occurs with a higher incidence rate in KTRs compared to the general population, at 9.6 and 6.6 cases per 10,000 patient-years, respectively.2,3 The incidence rate of cervical cancer in renal transplant patients is higher in both younger patients and those with a longer duration of immunosuppression therapy.4 Human papillomavirus (HPV) is the main aetiological factor in cervical cancer, and persistent HPV infection in the setting of immunosuppression is a significant risk factor for the development of cervical intraepithelial neoplasia (CIN) and cervical cancer in KTRs.5-8 Use of high-dose corticosteroids, in particular, increases the risk of HPV infection and persistence.9 Other risk factors for cervical cancer in renal transplant patients include older age at transplantation, high dose steroid use, smoking, and a history of CIN or cervical cancer before transplantation.9,10
Prevention strategies for cervical cancer in renal transplant patients include vaccination against HPV, cessation of smoking, and regular screening for CIN and cervical cancer. Guidelines recommend HPV vaccination for all renal transplant patients before transplantation, or as soon as possible after transplantation in both male and female patients aged <45 years, with the HPV9 vaccine currently recommended in Irish guidelines.11,12 However, the efficacy of the vaccine may be reduced in immunosuppressed patients, and the optimal timing and dosing of the vaccine in this population are still unclear.13 To the authors’ knowledge, no data are currently available regarding the uptake of this vaccine in KTRs in Ireland. Internationally, a low HPV vaccination rate is reported in some small studies of KTRs, varying from 4–32%, with a lack of awareness regarding the importance of vaccination commonly identified.14,15
Regular screening for CIN and cervical cancer is essential for the early detection and treatment in KTRs. Historical international guidelines recommended annual cervical cytology screening for female renal transplant patients.16-18 The Irish cervical screening programme, which moved from Pap smear cytology screening to HPV testing in March 2020, currently recommends screening take place within 1 year of kidney transplantation and then on an annual basis thereafter for patients with a negative HPV test between the ages of 25–65 years old.19 This annual HPV screening recommendation in Ireland had changed in the 2020 screening eligibility guidelines (Version 8), recommending that KTRs with a negative HPV test should undergo the standard HPV screening algorithm (i.e., screening every 3 years for ages 25–29 years and every 5 years for ages ≥30 years for patients with a negative HPV test). In 2021, the recommendation reverted to annual cervical screening for post-transplant recipients, even those with a negative HPV result. Little is known about the uptake of cervical screening in Irish KTRs in the current era. Previous studies, conducted prior to a well-established national cervical screening programme, suggested that uptake of screening in this region was very low.20,21
AIMS
In this study, the author sought to identify adherence with cervical screening and the prevalence rate of HPV vaccination in KTRs, and also to identify what patient-level barriers may exist to improving adherence with recommendations.
METHODS
Study Design, Setting, and Participants
A retrospective cohort study was conducted in a single centre to target two groups: firstly, all female KTRs ≤65 years regarding cervical screening, and secondly, all KTRs ≤45 years regarding HPV vaccination status. A cut-off age of 65 years was used for cervical screening in line with Irish cervical screening guidelines. Patients with a prior hysterectomy were excluded. A cut-off age of 45 years was used for the HPV vaccination group, as Irish vaccination guidelines recommend all KTRs ≤45 years should receive the HPV9 vaccine.
Data Collection and Analysis
Telephone consultations were conducted by junior doctors, unknown to the KTRs, to ascertain patient adherence with cervical screening, knowledge of screening recommendations, self-reported occurrence of an abnormal screening test, HPV vaccination status, and any patient-perceived barriers in adhering to recommended practice. KTRs of less than 12 months vintage or prior hysterectomy were excluded from the female patient ≤65 years cohort. No previously validated questionnaires were available to the research team for these purposes. Data collection took place from June–October 2022. Descriptive statistics, including cohort means, SD, and percentages were utilised to summarise the study results.
Ethical Approval
Ethical approval was granted by the local Research Ethics Committee. Informed consent was obtained from all participants.
RESULTS
Cervical Screening Survey
From a total cohort of 337 KTRs in the authors’ centre, there were 217 female KTRs ≤65 years old. Of these, 42 patients agreed to participate and three were excluded for a previous hysterectomy. Of the 39 included patients, the mean age was 45.3 years (SD: 10; median age: 44 years; SD: 10.6) and the mean transplant vintage was 123.6 months (SD: 86.2). The responses to the survey are summarised in Table 1. Since the time of transplantation, 34 patients (87%) had undergone a cervical screening and all of these patients reported attending screening whenever reminded or invited to do so by the cervical screening programme. There were five patients (13%) who had not attended cervical screening since the time of transplantation, and two of those indicated that the reason was that they had not received any communication from the cervical screening programme. Awareness of a specific recommendation for annual cervical screening in post-transplant recipients was evident in 27 patients (69%). Abnormal cervical screening had been detected in 18 patients (46%) and all of those had undergone colposcopy and large loop excision of the transformation zone procedure. A diagnosis of CIN was reported by six patients (15%). No patient had received a diagnosis of a gynaecological cancer since transplantation.
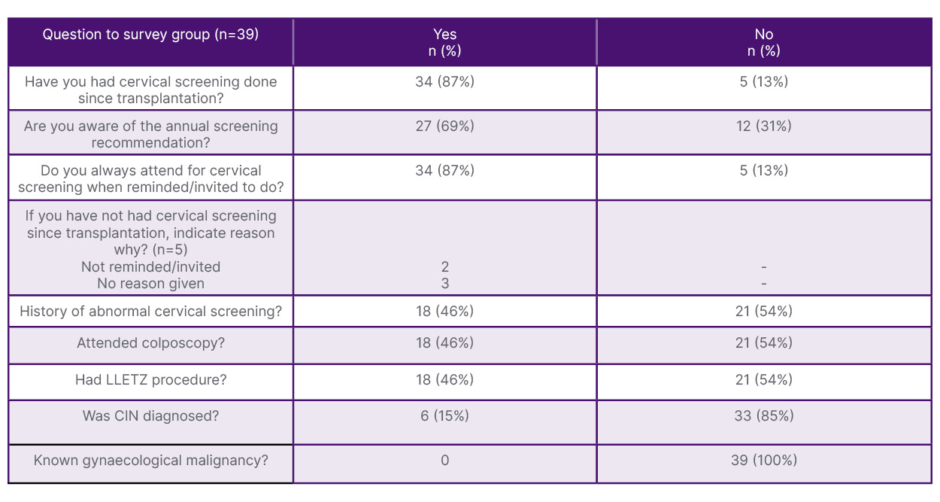
Table 1: Results of cervical screening questionnaire.
CIN: cervical intraepithelial neoplasia; LLETZ: large loop excision of the transformation zone.
HPV Vaccination Survey
From a total cohort of 337 KTRs in the authors’ centre, there were 48 KTRs who were ≤45 years old. Of these, 23 patients consented to participate in the telephone questionnaire. The mean age of this cohort was 37 years old (SD: 6.1) and the mean transplant vintage of this cohort was 86.3 months (SD: 60.4). HPV vaccination had been undertaken in five patients (22%) of the cohort (Table 2). There was awareness that KTRs have an increased risk of cancer over the course of their lifetime in 20 patients (87%), but only 9% of the cohort were aware that HPV vaccination could reduce the risk of cancer occurrence and only 4% were aware that HPV vaccination is recommenced by Health Service Executive (HSE) guidelines for KTRs either before or after transplantation. For unvaccinated KTRs (n=18), all patients stated that they would accept HPV vaccination if it was provided at their supervising hospital.
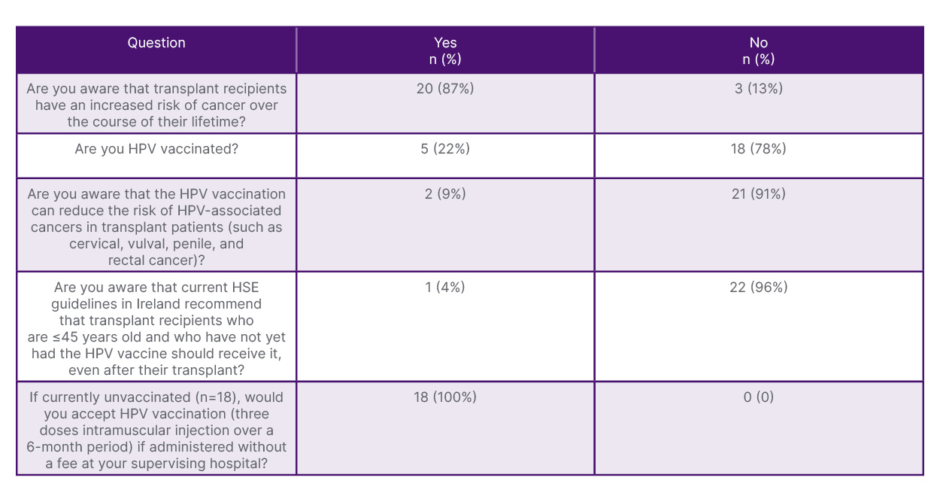
Table 2: Results of survey on HPV vaccination.
HPV: human papillomavirus; HSE: Health Service Executive.
DISCUSSION
In this contemporary KTR cohort, the authors identified that a high proportion of patients had attended cervical screening in line with national cervical screening guidelines. Some patients who had not undergoing screening identified a lack of notification from the cervical screening programme (“CervicalCheck”) as the reason for non-adherence. Abnormal cervical screening was commonly encountered, with 46% of this cohort having been sent forward for colposcopy following an abnormal screening test. In terms of HPV vaccination, either prior or post-transplantation, the prevalence of vaccination was low, at 22%. There was a low level of awareness regarding the importance of HPV vaccination in preventing cancer occurrence in KTRs.
IMPLICATIONS FOR PRACTICE
The current study suggests a much higher adherence with cervical screening recommendation in KTRs compared to the low uptake reported in a cohort of 64 female KTRs in another Irish centre in 2006, which demonstrated that just 16% were having regular screening.21 A study in Northern Ireland in 2009, using a questionnaire administered to 173 female KTRs, demonstrated that just 10% were adherent with recommended cervical screening.20 While acknowledging that the authors’ provocative findings are at risk of self-selection sampling bias, it is also certainly plausible that KTR engagement with cervical screening has improved since the era of those older studies. Firstly, the national CervicalCheck screening programme commenced in Ireland in 2008, with female patients between 25–65 years old being automatically identified from the Department of Social Protection records and periodically notified to arrange cervical screening. Secondly, there has been a high level of media coverage of the cervical screening programme in Ireland in recent years, due to investigations into missed diagnoses of abnormal tests. Taken together, it is likely that current KTRs would be more aware of the importance of cervical screening and of how to access it compared to their historical peers. However, as a retrospective cohort study, the authors’ findings and interpretations are subject to limitations, notably selection biases, recall biases, and other confounders, and must be viewed in this setting. A larger and nationwide survey of cervical screening, ideally directly accessing the CerivcalCheck register, would be desirable to corroborate the current findings.
The low level of HPV vaccination noted in the authors’ KTR cohort is reflective of findings at other international centres.14,15 The low level of awareness around the importance of HPV vaccination in cancer prevention and its recommendation by guidelines were also noted in the previous studies. There are multiple factors relating to this preventable gap in care, ranging from the focus of the medical team being on graft outcomes and more short-term goals, time constraints at medical visits, knowledge gaps in healthcare professionals regarding HPV vaccination, and reluctance to discuss sexual health by practitioners or patients. The vast majority of secondary level school-children in Ireland now receive HPV vaccination through the school immunisation programmes (girls since 2010 and boys since 2019), so it is expected that future generations of KTRs will already have received HPV vaccination prior to transplantation. A more prominent focus on HPV vaccination must be realised for current KTRs and current patients with advancing CKD who would not have been captured in the school immunisation programme. This study shows a high degree of willingness amongst KTRs to accept HPV vaccination if delivered conveniently through the hospital’s renal department. Importantly, delivery of hepatitis B vaccination is a long established practice in all renal units nationally for pre-dialysis and dialysis patients to protect patients and staff from the risk of blood-borne virus transmission. This practice occurs at no direct cost to the patient and the vaccine administration is typically aligned with patient’s scheduled visits to the hospital where possible. Hepatitis B vaccinations are supplied to Irish hospitals via the National Cold Chain Supply without a direct drug cost to the hospital. The authors are advocating locally that HPV vaccination can and should be delivered in a similar manner as a quality improvement initiative and cancer prevention strategy in KTRs.
STUDY LIMITATIONS
This study provides an important insight into the current era of cervical screening in KTRs and primary data on uptake of HPV vaccination in KTRs in Ireland. However, the study is limited by the possibility of self-selection bias and other outlined biases associated with retrospective cohort studies. The small cohort number and the single-centre design also reduce the generalisability of the results. It is also acknowledged that non-validated and locally developed questionnaires were utilised for data collection. This can be associated with measurement error and the data should be interpreted accordingly, but the use of such questionnaires continues to have a role in studies where no validated tool exists and where low-cost, rapid, and tailored patient data are required.
CONCLUSION
This study suggests a significant improvement in the uptake of cervical screening in KTRs in Ireland in the current era, but validation in a larger and multicentre cohort is desirable. Ongoing education on the importance of cervical screening and HPV vaccination for KTRs is paramount. This should be led by healthcare professionals in the transplant clinic setting, using quality improvement initiatives to harness the known preventive strategies that exist to improve outcomes for KTRs in terms of HPV-associated cancers.






