Abstract
AI has transitioned from experimental promise to real-world clinical application across diagnostics, therapeutics, and healthcare delivery. Advances in imaging analysis, predictive analytics, and multimodal data integration now support earlier diagnosis, personalised treatment selection, and proactive disease monitoring. Despite strong technical performance, real-world impact remains limited by data quality, interoperability, governance, workflow integration, and clinician trust. This article reviews current applications of AI across medical specialties, highlights emerging use cases in treatment response prediction and remote monitoring, and examines barriers to implementation. It argues that future impact will depend less on algorithmic innovation and more on clinical integration, human–AI collaboration, regulation, and system-level redesign to ensure safe, equitable, and scalable adoption.
Key points
1. AI is increasingly embedded in healthcare, addressing rising data complexity, workforce pressures, and the need for earlier, more personalised diagnosis and treatment.2. This is a narrative review examining current and emerging applications of AI in diagnostics, treatment response prediction, remote monitoring, and clinical decision-making across multiple specialties.
3. AI can enhance clinical precision and efficiency, but meaningful impact depends on integration into workflows, strong governance, clinician leadership, and a focus on trust, equity, and human–AI collaboration, rather than algorithmic performance alone.
INTRODUCTION
Over the past decade, AI has moved from conceptual promise to real-world clinical application. Advances in deep learning, natural language processing, and multimodal data integration have enabled AI systems to interpret medical imaging, predict treatment response, stratify risk, and automate workflows at scale.1 Algorithms now routinely classify radiographs, flag diabetic retinopathy, segment tumours on MRI, transcribe consultations, and predict hospital deterioration.2 However, while technical performance has accelerated, real-world clinical impact has been slower and more fragmented. Translation into routine care remains uneven, constrained by data quality, governance, clinician trust, interoperability, and equity.3 Healthcare is fundamentally a socio-technical system, and accuracy alone does not guarantee adoption, safety, or value. Successful AI deployment requires alignment with workflows, governance, regulatory frameworks, clinician trust, patient acceptability, and health-system incentives.4 This article explores how AI is reshaping diagnostics and therapeutics across medical specialties using imaging, predictive analytics, and real-world deployment as core examples. It argues that the next phase of impact will depend less on algorithmic novelty and more on clinical integration, validation, human–AI collaboration, and system-level redesign.
AI IN DIAGNOSTICS
AI is already transforming diagnostic pathways across multiple therapy areas, with growing evidence of improved early detection and risk stratification (Table 1). Medical imaging has been the earliest and most mature application of AI in healthcare. Deep learning systems have demonstrated specialist-level performance in detecting breast cancer on mammography, lung cancer on CT imaging, and multiple pathologies across radiographic modalities. For example, an AI system for breast cancer screening demonstrated performance comparable to that of radiologists while reducing workload by approximately 44% in a retrospective evaluation, highlighting potential efficiency gains.5 Similarly, deep learning-based lung cancer screening models have shown reductions in false positives compared to traditional approaches.6
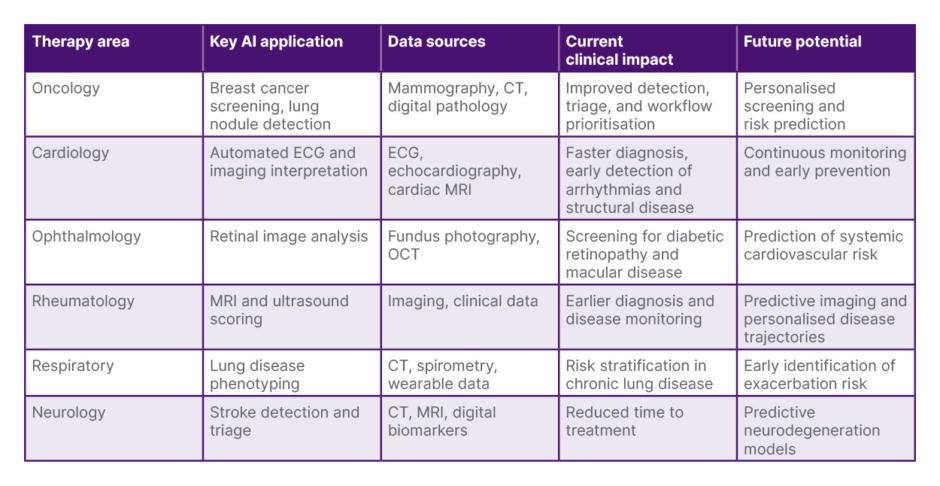
Table 1: Clinical applications of AI in diagnostics across therapy areas.5-7
AI is increasingly used in diagnostic imaging to support early detection, improve consistency, and optimise clinical workflows. Deep learning and multimodal approaches are expected to enhance predictive and personalised diagnostics across specialties.
OCT: optical coherence tomography.
In digital pathology, AI systems increasingly support tumour classification, biomarker quantification, and prognostication.7 Clinical value often lies not in replacing clinicians but in reducing cognitive load, improving consistency, accelerating turnaround time, and reducing diagnostic variation. AI triage systems can flag abnormal scans for urgent review, reducing time-to-treatment for stroke, trauma, and oncological care. Beyond accuracy, AI is reshaping workflow. Automated prioritisation, structured reporting, and decision support tools may help address workforce shortages and rising imaging demand. As chronic disease prevalence increases, scalable diagnostic capacity is becoming essential.
Ultrasound represents another particularly promising frontier. Operator dependency, variable image quality, and training constraints have historically limited scalability. AI-guided acquisition systems now assist probe positioning, optimise image quality, and automate anatomical recognition, supporting non-expert users in acquiring clinically meaningful images. In inflammatory arthritis and musculoskeletal medicine, AI-assisted ultrasound interpretation has demonstrated potential to standardise scoring, reduce inter-observer variability, and support earlier diagnosis. Similar approaches are expanding in emergency medicine, cardiology, obstetrics, and respiratory care. The next evolution moves beyond single-modality AI towards multimodal fusion, combining imaging, laboratory data, genomics, wearable signals, electronic health records, and patient-reported outcomes. Such systems can contextualise imaging findings within longitudinal clinical trajectories, improving predictive accuracy and reducing false positives. Multimodal AI may also support earlier identification of disease in at-risk populations. By analysing subtle patterns across multiple data streams, these models could detect preclinical disease and enable preventive intervention.
PREDICTING TREATMENT RESPONSE
Across many specialties, treatment selection remains challenging and is driven largely by population averages from clinical trials rather than individual biology or behaviour. Machine learning models can integrate high-dimensional clinical data, imaging features, and molecular signatures to stratify patients by likelihood of benefit or toxicity.8 In oncology, radiomic signatures increasingly guide immunotherapy and targeted therapy selection. In chronic inflammatory diseases, predictive models are emerging that estimate response to biologic and targeted synthetic therapies using baseline disease activity, comorbidities, imaging features, and longitudinal digital biomarkers. These developments are driving a shift towards precision and proactive care across specialties (Table 2).
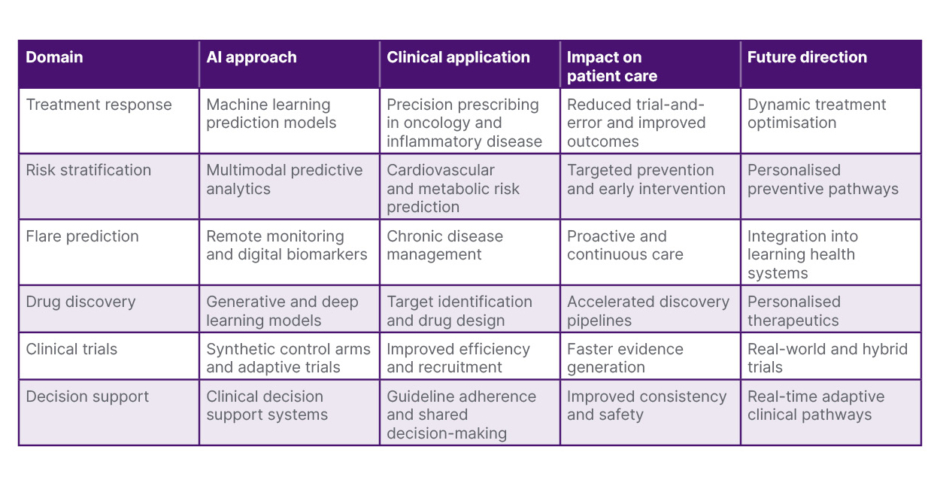
Table 2: AI in therapeutics and precision medicine.2,8,9
AI is enabling precision medicine through treatment prediction, risk stratification, and remote monitoring. These approaches may improve outcomes, support personalised care pathways, and accelerate research and drug development.
An important next step is the integration of predictive models into routine clinical decision-making. Rather than producing static probability scores, future systems may provide adaptive recommendations that evolve as new patient data become available. For example, treatment response models could update predictions based on early changes in symptoms, laboratory results, or digital biomarkers, allowing more rapid optimisation of therapy. This dynamic approach reflects how clinicians already think in practice, but may improve precision and reduce delays in achieving disease control. Importantly, these tools may also support shared decision-making. Patients increasingly expect personalised explanations of treatment benefits and risks. AI systems could help visualise outcomes in ways that align with individual priorities, such as symptom control, long-term safety, work participation, and quality of life. This may strengthen communication and trust between clinicians and patients.
FLARE PREDICTION AND REMOTE MONITORING
Chronic disease trajectories are dynamic, and flares, defined as an increase in disease activity, are often unpredictable. AI-enabled remote monitoring platforms integrate wearable data, patient-reported outcomes, and physiological signals to predict deterioration or flare before clinical escalation is required. In cardiology and respiratory medicine, predictive models anticipate decompensation days in advance. For example, in heart failure, continuous wearable monitoring combined with predictive analytics has been associated with earlier detection of decompensation and reduced hospitalisation risk in prospective studies.10 Similar approaches are emerging in rheumatology, diabetes, and neurological conditions, enabling anticipatory care rather than reactive care. Remote monitoring supports new models such as virtual clinics, patient-initiated follow-up, and proactive outreach. These approaches may improve patient experience while reducing unnecessary healthcare utilisation.
These strategies may also support personalised follow-up pathways. Patients at low risk of deterioration could be monitored remotely, while those at higher risk receive earlier clinical review. Over time, this model may enable a shift towards continuous care rather than episodic care. Furthermore, digital monitoring may empower patients to take a more active role in managing their conditions. More advanced systems simulate patient trajectories under different therapeutic strategies. These digital twin approaches allow scenario testing and optimisation of treatment strategies, but require careful validation, transparency, and governance.
REAL-WORLD DEPLOYMENT
AI performance is constrained by fragmented, incomplete, and biased healthcare data. Interoperability across hospital systems, community care, imaging platforms, and patient-generated data remains a major barrier to scalability. Clinicians adopt tools that improve efficiency and demonstrably improve outcomes. Black-box systems that disrupt workflows or generate excessive alerts rapidly lose credibility. Clear accountability frameworks are essential when AI recommendations influence clinical decisions. Regulatory frameworks are evolving to address adaptive algorithms, post-market surveillance, and algorithm drift management. Prospective validation and health-economic assessment remain essential. Bias in training data can propagate health inequities if not proactively mitigated. Digital exclusion also risks widening disparities unless addressed through inclusive design and policy. Addressing these barriers is essential to ensure safe, equitable, and scalable deployment of AI in healthcare (Table 3).
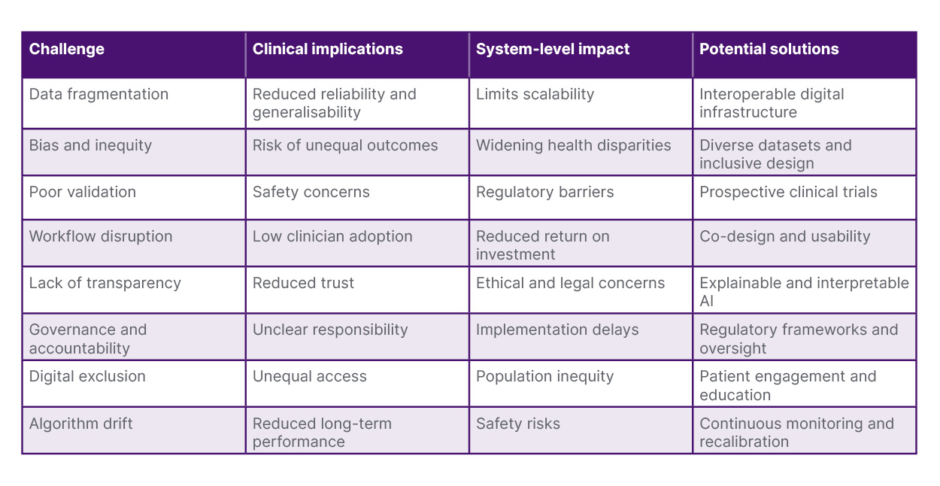
Table 3: Barriers and enablers for real-world implementation of clinical AI.3,4,9
Real-world implementation requires alignment of technology, clinical workflows, governance, and patient engagement. Key barriers to clinical adoption include bias, poor validation, workflow integration, and data fragmentation. Addressing these challenges through governance, regulation, and stakeholder engagement is essential for safe and equitable implementation.
In digital pathology, AI systems increasingly support tumour classification, biomarker quantification, and prognostication.7 Clinical value often lies not in replacing clinicians but in reducing cognitive load, improving consistency, accelerating turnaround time, and reducing diagnostic variation. AI triage systems can flag abnormal scans for urgent review, reducing time-to-treatment for stroke, trauma, and oncological care. Beyond accuracy, AI is reshaping workflow. Automated prioritisation, structured reporting, and decision support tools may help address workforce shortages and rising imaging demand. As chronic disease prevalence increases, scalable diagnostic capacity is becoming essential.
HUMAN–AI COLLABORATION
AI is unlikely to replace clinicians, but will redefine professional roles. Routine pattern recognition and administrative tasks will increasingly be automated, allowing clinicians to focus on complex judgement, shared decision-making, and leadership. Training curricula must evolve to include data literacy, AI governance, and digital leadership competencies. Clinicians will increasingly need to understand not only how to use AI tools but also how to evaluate their performance, recognise bias, and ensure safe, equitable implementation. This represents a shift from passive users of technology towards active stewards of digital innovation. The future workforce will also become more interdisciplinary. Collaboration between clinicians, data scientists, engineers, behavioural scientists, and policymakers will be essential to co-design solutions that are clinically relevant and socially acceptable. Patient and public involvement will be equally important to ensure transparency, trust, and alignment with patient values. These partnerships may foster new models of care that are more adaptive, personalised, and responsive.
Although adoption varies across specialties, shared infrastructure increasingly underpins diverse use cases, including imaging platforms, predictive analytics engines, and language models.9 This convergence enables faster translational impact across therapy areas. Human oversight remains central. AI identifies patterns but cannot fully interpret context, values, or preferences. Shared decision-making, ethical judgement, and compassionate care will therefore remain fundamental. The goal is not automation alone but augmentation, where intelligent systems support clinicians in delivering more precise, proactive, and patient-centred care.
FUTURE DIRECTIONS
Over the past 2 decades, structural changes in healthcare have created the conditions necessary for AI deployment. The widespread adoption of electronic health records has digitised clinical workflows at scale. At the same time, wearable technologies, advanced imaging, genomic sequencing, and remote monitoring have generated unprecedented volumes of digital health data. National biobanks containing hundreds of thousands of participants have enabled high-dimensional population-level modelling. Meanwhile, diagnostic and therapeutic pathways have become increasingly complex, often exceeding the cognitive bandwidth of individual clinicians. AI has therefore emerged not merely as a technological innovation, but as a response to increasing data density and clinical complexity.
The next decade will likely be characterised by integrated multimodal intelligence, continuous learning systems embedded in care pathways, regulatory maturity, stronger clinician leadership, and an explicit focus on equity and trust. Rather than isolated tools, AI will increasingly operate as part of connected digital ecosystems, linking primary care, specialist services, community care, and patient-generated data. This convergence may enable real-time risk stratification, dynamic treatment optimisation, and earlier intervention across a wide range of conditions.
In digital pathology, AI systems increasingly support tumour classification, biomarker quantification, and prognostication.7 Clinical value often lies not in replacing clinicians but in reducing cognitive load, improving consistency, accelerating turnaround time, and reducing diagnostic variation. AI triage systems can flag abnormal scans for urgent review, reducing time-to-treatment for stroke, trauma, and oncological care. Beyond accuracy, AI is reshaping workflow. Automated prioritisation, structured reporting, and decision support tools may help address workforce shortages and rising imaging demand. As chronic disease prevalence increases, scalable diagnostic capacity is becoming essential.
Continuous learning systems represent a particularly important shift. By integrating real-world data into routine care, these platforms could refine clinical pathways and improve outcomes over time. In this model, healthcare becomes adaptive, with feedback loops supporting ongoing improvement rather than static guideline-driven practice. Such approaches may be especially valuable in chronic disease, multimorbidity, and ageing populations, where complexity and variability challenge traditional models of care. Large language models are already beginning to support clinical documentation, triage, and knowledge synthesis at scale. Over time, these tools may enhance communication between clinicians and patients, support shared decision-making, and facilitate personalised education. They may also accelerate research through improved literature synthesis, protocol development, and trial design.
At a broader level, AI may support prevention and population health by identifying individuals at high risk and enabling earlier intervention. This could include targeted screening, lifestyle interventions, and community-based care. Beyond incremental integration, AI may drive more fundamental shifts in healthcare delivery. One potential transformation is the decentralisation of diagnosis, with AI-enabled point-of-care tools moving assessment from hospitals into community settings. Continuous risk modelling may replace episodic appointments with dynamic, data-driven care pathways. In therapeutics, adaptive treatment algorithms could evolve in near real time as population-level outcomes are updated, challenging traditional guideline cycles. Conversely, it is also plausible that AI remains largely assistive rather than transformative, constrained by regulatory, ethical, and reimbursement realities. Whether AI radically reshapes care or becomes a sophisticated decision-support layer will depend less on technical capability and more on governance, trust, and system redesign.
As health systems shift towards value-based and preventive care, such capabilities may become increasingly important. However, equity must remain central. Without careful design, AI risks reinforcing existing disparities through biased datasets, digital exclusion, or unequal access to innovation. Conversely, when implemented thoughtfully, these technologies offer an opportunity to improve access, reduce unwarranted variation, and support more consistent care across regions and populations. Public engagement, transparency, and co-design will therefore be essential to maintain trust and ensure that AI-driven transformation benefits all.
CONCLUSION
AI is reshaping diagnostics and therapeutics, but real impact depends on integration, governance, trust, and equity rather than algorithmic performance alone. When deployed thoughtfully, AI augments human expertise, accelerates learning, and enables personalised, proactive care at scale. The future of AI in medicine will be defined by partnership between clinicians, patients, and intelligent systems. If guided by strong clinical leadership and public trust, this transformation offers an opportunity to improve outcomes, experience, and sustainability across health systems.






