BACKGROUND AND AIMS
Fibrosis-4 (FIB-4) screening for people with Type 2 diabetes (T2D) is recommended;1,2 however, screening and hepatology linkage for high-risk individuals remain a challenge. The authors integrated a reflexive MASLD fibrosis screening algorithm and referral pathway into iDiabetesPlus, a precision diabetes care platform being trialled in primary care in Scotland.3
Here, the authors present the key MASLD screening results from the first year of the iDiabetes study.
METHOD
iDiabetesPlus was implemented from 28 October 2024 in 16 primary care practices in Tayside, Scotland. All people with diabetes are automatically enrolled on iDiabetesPlus at their annual diabetes review. Automated FIB-4 screening is performed for all patients. FIB-4 is stratified as: low risk: <1.30 (aged <65 years)/ <2.0 (aged ≥65 years); intermediate risk: 1.30–2.67 (aged <65 years)/2.0–2.67 (aged ≥65 years); and high risk: >2.67. If alanine aminotransferase (ALT) >30, additional liver aetiological screening is performed, with reflexive enhanced liver fibrosis (ELF) testing in indeterminate or high-risk FIB-4. Automated referral to secondary care is generated for those with ALT ≤30 and FIB-4 >2.67; or ALT >30 and ELF ≥9.8, or FIB4 >3.25, or positive aetiology results. For all enrolled patients, iDiabetesPlus generates comprehensive diabetes and MASLD management recommendations for primary care practitioners and patients, and guidance on the timing of interval FIB-4 testing.
RESULTS
From 28th October 2024–31st December 2025, 4,695 people with T2D enrolled in iDiabetesPlus. Of these 1,954 (41.6%) were female, median age of 68.0 years (range: 18–98), BMI of 31.0 kg/m2, and HbA1c of 58.0 mmol/mol. ALT was ≤30 in 67.5% (n=3,170) and >30 in 32.5% (n=1,524). 99.3% (n=4,662) received successful FIB-4 screening. Most patients (n=3,913; 83.9%) had low-risk FIB-4, with advice to repeat FIB-4 in 2 years (Figure 1). Five hundred and sixty-nine (8.8%) had intermediate risk, with advice on optimising metabolic health and repeating FIB-4 in 12 months.
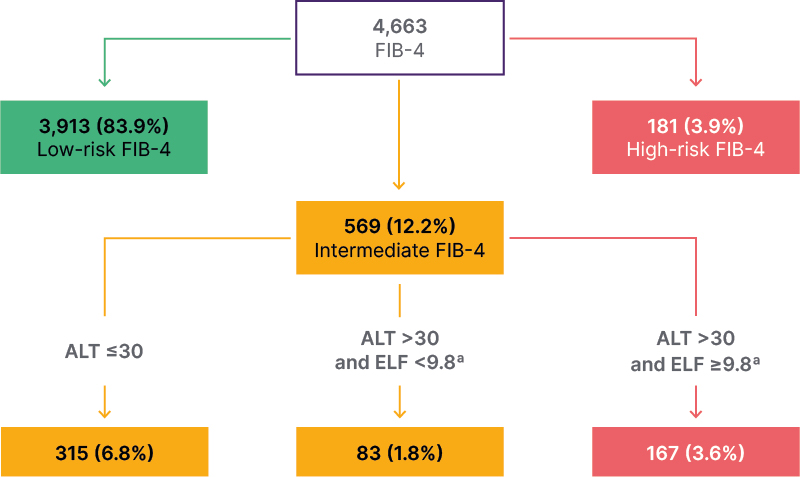
Figure 1: Schematic of FIB-4 results and categorisation.
ªMissing ELF n=4.
FIB-4 and ELF distribution of screened patients (NAFLD Fibrosis Score not shown here for clarity).
FIB-4 is stratified as: low risk: <1.30 (aged <65 years)/<2.0 (aged ≥65 years); intermediate risk: 1.30-2.67 (aged <65 years)/2.0-2.67 (aged ≥65 years); and high risk: >2.67.
Advice to GP and patient for repeat FIB-4 in 2-3 years (green box). Advice to GP and patient on how to optimise metabolic health and repeat FIB-4 in 1 year (yellow box). Automated referral to secondary care hepatology for further assessment (red box).
ELF: enhanced liver fibrosis; FIB-4: fibrosis-4; GP: general practitioner.
Of the 250 (5.3%) patients with T2D who received ELF testing, 83 (33.2% of ELF) were <9.8, and 167 (66.8%) had an ELF score ≥9.8. Three hundred and forty-eight (7.4%) patients with T2D were eligible for Fibroscan, with 258 (5.5%) receiving a scan. One hundred and three patients had
a liver stiffness measurement (LSM) ≥10 kPa (2.2% of enrolled patients), and 57 patients had LSM >15 kPa (1.2% of all enrolled patients).
A diagnosis of MASLD was made in 190 (69.6%) patients seen in clinic, metabolic and alcohol related liver disease in 31 (11.4%) and alcohol related liver disease in 1 (0.4%). No liver disease was identified in 42 (15.4%) patients, and other/mixed aetiology liver disease in 9 (3.3%) patients. One new chronic HBV and eight new haemochromatosis diagnoses were identified. Three patients were found to have hepatocellular carcinoma at the time of initial liver assessment. Just over half (n=146; 53.5%) of patients were discharged back to primary care following their index clinic assessment.
CONCLUSION
Automated MASLD screening within the precision iDiabetesPlus platform results in near universal FIB-4 screening in a real-world primary care T2D population. Over 80% of FIB-4 screening is low-risk, meaning patients can safely be managed in primary care, with automated advice on MASLD management and interval FIB-4 testing generated for clinicians and patients. Targeted ELF testing reduced the need for Fibroscan and secondary care review by almost a third in those tested. The authors identified possible new compensated advanced chronic liver disease (LSM >10 kPa) in 2.2% of all patients screened for T2D. >50% of patients assessed in the clinic were discharged after their initial review.