BACKGROUND AND AIMS
Metabolic dysfunction-associated steatotic liver disease (MASLD) is increasingly recognised as a systemic disorder driven by cardiometabolic risk factors (CMRF), including obesity, Type 2 diabetes mellitus (T2DM), hypertension, and dyslipidaemia.1-3 While advanced fibrosis (AF) is a major determinant of hepatocellular carcinoma (HCC) risk, the impact of cumulative metabolic burden and specific CMRF combinations on HCC trajectories remains unclear.2,3 This study aimed to evaluate how distinct metabolic profiles influence HCC risk in patients with MASLD with AF.
MATERIALS AND METHODS
In this Italian cohort study, patients with MASLD-AF were stratified into clusters based on the number and combination of CMRFs (from one to four). Individual metabolic dysfunction profiles were defined through non-redundant permutations of CMRFs.4 The primary endpoint was 5-year HCC incidence, while secondary endpoints included HCC staging at diagnosis (Milan-out criteria)5 and identification of high-risk metabolic profiles. Multivariable competing risk models adjusted for demographic and clinical variables were applied.
RESULTS
A total of 1,921 patients were retrospectively analysed after exclusions. Increasing metabolic burden was associated with worsening inflammatory and metabolic parameters. Patients with ≥3 CMRFs (Cluster III and IV) exhibited a significantly higher risk of HCC compared with lower-burden clusters (odds ratio: 2.81; 95% CI: 1.345–3.211). Moreover, cumulative metabolic burden correlated with more advanced tumour stage at diagnosis (odds ratio: 2.46; 95% CI: 1.226–3.035; p=0.0162; Figure 1).
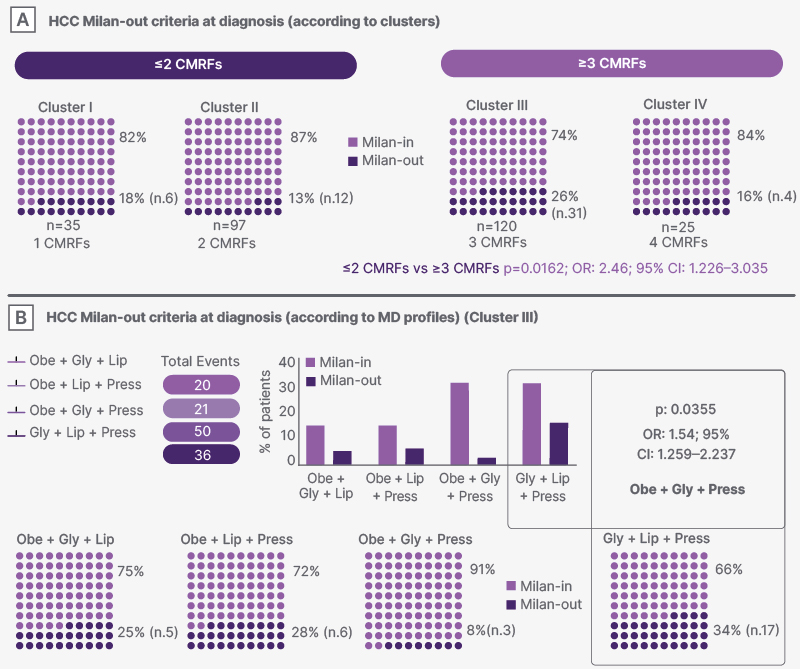
Figure 1: Hepatocellular carcinoma risk according to metabolic clusters and individual metabolic dysfunction profiles.
Risk of HCC stratified by cumulative metabolic burden and specific MD profiles in patients with MASLD and AF.
Panel A shows the risk of advanced HCC at diagnosis according to metabolic clusters defined by the number of CMRFs. A progressive increase in HCC risk is observed with increasing metabolic burden.
Panel B illustrates the risk of advanced HCC at diagnosis according to individual MD profiles, highlighting heterogeneity within clusters based on specific combinations of CMRFs. Selected profiles, particularly those including T2DM, obesity, and hypertension, are associated with higher HCC risk.
AF: advanced fibrosis; CMRF: cardiometabolic risk factors; Gly: impaired glucose metabolism/diabetes mellitus; HCC: hepatocellular carcinoma; HR: hazard ratio; Lip: dislipidaemia; MASLD: metabolic dysfunction-associated steatotic liver disease; MD: metabolic dysfunction; Obe: obesity; OR: odds ratio; Press: arterial hypertension; T2DM: Type 2 diabetes mellitus; vs: versus.
Among specific profiles, the combination of T2DM, obesity, and hypertension conferred the highest HCC risk (odds ratio: 2.24; 95% CI: 1.562–2.985; p<0.001), including increased likelihood of Milan-out criteria tumours (odds ratio: 1.541; 95% CI: 1.259–2.237; p=0.035; Figure 1). Importantly, dynamic changes in metabolic status influenced disease trajectories: incident T2DM during follow-up acted as a disease-modifying event. Mediation analysis demonstrated that up to 82% of the association between metabolic burden and HCC risk was driven by diabetes onset, suggesting a central mechanistic role.
CONCLUSION
Distinct cardiometabolic profiles define heterogeneous HCC risk in patients with MASLD-AF. Risk is not solely determined by the number of CMRFs but by their specific combinations and dynamic interactions.2 In particular, T2DM emerges as a key mediator linking metabolic burden to carcinogenesis.2 These findings support a precision medicine approach, where individual metabolic signatures enable tailored HCC risk stratification and surveillance strategies.5






