Author: *Maja Thiele1,2
1. Department of Clinical Research, University of Southern Denmark, Odense, Denmark
2. Evido Health, Copenhagen, Denmark
*Correspondence to [email protected]
Disclosure: Thiele has received speaker’s fees from Echosens, Madrigal, and Novo Nordisk; advisory fees from AstraZeneca and GSK; and is Co-founder and full-time employee of Evido Health.
Keywords: MASLD, metabolic dysfunction-associated steatohepatitis (MASH), non-invasive test (NIT), vibration-controlled transient elastography (VCTE; Echosens, Paris, France).
Citation: EMJ Hepatol. 2026;14[1]:33-37. https://doi.org/10.33590/emjhepatol/B9064DI8
![]()
The postgraduate course kicked off the theme with its devotion to diagnostics in liver diseases and sessions covering broad topics such as histology, imaging, blood-based testing, and future technologies. The dedicated MASLD session made especially clear that the approval of semaglutide and resmetirom as pharmaceutical interventions for pre-cirrhotic metabolic dysfunction-associated steatohepatitis (MASH) has created a need for highly accurate biomarkers that support clinical care beyond cross-sectional diagnosis, extending into prediction, monitoring, and stopping rules.
However, many hepatologists remain anchored to past practices. This became clear in Isabel Graupera’s, Hospital Clinic de Barcelona, Spain, talk on moving beyond Fibrosis-4 (FIB-4), where audience voting captured a discordance: one-third of attendees still viewed FIB-4 as an ideal rule-out test because of its high negative predictive value (NPV), whereas a 58% majority supported the more cautious, correct position that FIB-4 may be useful as a first-line tool but needs second-line confirmation. Graupera highlighted that FIB-4’s suboptimal sensitivity means the test will miss many cases, despite its high NPV.1 In low-prevalence settings, a high NPV is almost inevitable: if disease prevalence is 5%, even a coin toss would have an NPV of 95%. She then discussed newer multivariable tools developed for screening in general populations (CIRRhosis Using Standard tests [CIRRUS], LiverRisk score, CORE, Chronic Liver Disease [CLivD]), at-risk MASLD populations (Metabolic Dysfunction-Associated Fibrosis 5 [MAF-5] and Steatosis-Associated Fibrosis Estimator [SAFE]), and across the steatotic liver disease spectrum (LiverPRO, Evido Health, Copenhagen, Denmark).
Laurent Castera’s, Université Paris-Cité, France, subsequent presentation on patient selection for MASH pharmaceutical therapy placed NITs at the centre.2 He highlighted data from the LiverScreen study suggesting that approximately 2.0% of the screened population would be eligible for treatment using a vibration-controlled transient elastography (VCTE; Echosens, Paris, France) range of 10–20 kPa. These data underscore both the opportunity for treatment, but also the future workload for hepatologists, if population-level case finding is broadly implemented.
The last day of the Congress included the multisociety initiatives session that elegantly looped back to the postgraduate course theme. Frank Tacke, Charité – Universitätsmedizin Berlin, Germany, presented the updated EASL–European Association for the Study of Diabetes (EASD)–European Association for the Study of Obesity (EASO) guidance on MASH-targeted pharmacotherapy, where NITs are now recommended to support treatment initiation, monitor response, and help decide whether therapy should be continued or considered futile.3 Figure 1 sums up main points on how patients with MASH may be detected in primary care, referred for subsequent confirmative testing in specialist care, started on pharmaceutical treatment, and moni
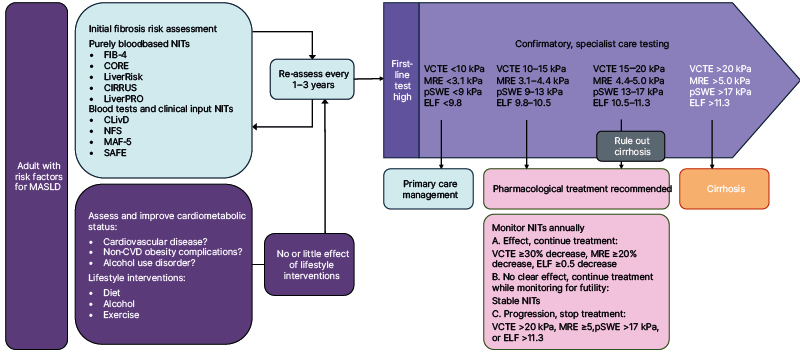
Figure 1: Biomarker strategies to select patients for MASLD therapies, based on presentations at the EASL
Adapted from presentations at the EASL Congress 2026.1,3
The treatment algorithm is adapted from the presentation of the updated EASL–EASD–EASO guidance. This guidance had not been published in full at the time of writing and may therefore change after review. pSWE was not included in the figure presented during the multisociety initiatives session, but was added by the author, interpreted according to the WFUMB-endorsed ‘rule of four’. The original figure also presented a lower ELF threshold of 9.2; the author has assumed that this was a typographical error.
CIRRUS: Cirrhosis Risk Score; CLivD: Cross-Liver Disease score; CORE: Composite Risk Evaluation score; CVD: cardiovascular disease; EASD: European Association for the Study of Diabetes; EASL: European Association for the Study of the Liver; EASO: European Association for the Study of Obesity; ELF: Enhanced Liver Fibrosis (test/score); FIB-4: Fibrosis-4 Index; LiverPRO: Liver Prognostic Risk Outcome score (Evido Health, Copenhagen, Denmark); LiverRisk: Liver Risk score; MAF-5: Metabolic Dysfunction-Associated Fibrosis-5 score; MRE: magnetic resonance elastography; NFS: non-alcoholic fatty liver disease Fibrosis Score; NIT: non-invasive tests; pSWE: point shear wave elastography; SAFE: Steatosis-Associated Fibrosis Estimator; VCTE: vibration-controlled transient elastography.
Following the postgraduate course, the scientific programme included several newsworthy sessions revealing three overall themes of biomarker use: longitudinal NITs for monitoring, added accuracy by combining tests, and revealing a divide between what is recommended by guidelines, and what is implemented in clinical care.
REDEFINING BIOMARKER USAGE FROM SINGLE SNAPSHOTS TO LONGITUDINAL TRENDS
Many of the biomarker-centred studies presented a shift from one-off diagnostic evaluation towards longitudinal NITs for monitoring and early prediction of pharmacodynamic effect. Data from the MAESTRO-NASH Phase III resmetirom trial showed that reductions in alanine aminotransferase (ALT) at Week 12, MRI-proton density fat fraction and magnetic resonance elastography at Week 16, and PRO-C3 at Week 24 correlated with histological MASH resolution and fibrosis improvement at end-of-study after 52 weeks.4 This indicates that early changes in NITs can be used as indicators for long-term treatment response. In the 2-year open-label extension of the MAESTRO-NAFLD-1 trial of 180 patients with compensated cirrhosis, nearly half (49.3%) exhibited a significant response according to the ANTICIPATE-NASH model (VCTE, platelet count, and BMI), indicating improvement in clinically significant portal hypertension, albeit without liver vein catheterisation to confirm actual portal pressure improvement.5
NITs for monitoring in low prevalence settings perform very differently from monitoring in MASH trial patients with high prevalence of advanced fibrosis. On Saturday, Jesse Pustjens, Erasmus MC, Rotterdam, the Netherlands, and colleagues from the European LiverScreen consortium, presented data from community-based liver stiffness screening programmes in 4,538 participants.6 Here, only 38% of the 251 participants with elevated VCTE ≥8 kPa at baseline had persistently elevated VCTE elevation at the repeat visit after a median follow-up of 4.3 years. However, combination with other NITs improved the ability to detect persistent elevation in VCTE: among individuals with elevated baseline VCTE but low FIB-4, LiverPRO, LiverRisk, or MAF-5, transient VCTE elevation rates were high, ranging from 81% (LiverPRO) to 74% (FIB-4). Conversely, when baseline NIT-scores were high, persistent VCTE elevation rates ranged from 43% (LiverPRO) to 47% (MAF-5). These findings underscore the importance of combining different NITs to improve fibrosis case finding in low prevalence settings.
FROM CONCOMITANT TESTING TO FAILED REAL-WORLD IMPLEMENTATION
The advantage of moving from single-test interpretation towards combined NIT strategies extends beyond screening populations. In endocrinology patients with a BMI exceeding 35 kg/m² and a 30% prevalence of significant fibrosis based on magnetic resonance elastography ≥3.3 kPa, Ajmera et al.7 showed that combining VCTE ≥8 kPa with Enhanced Liver Fibrosis (ELF; Siemens Healthineers, Erlangen, Germany) score ≥9.2 lowered the false-positive rate to 9%. Discordant results also hold valuable information: in a prospective MASLD cohort, approximately half of patients with VCTE ≥8 kPa had discordant ELF <9.8.8 Such discordance was commonly associated with abdominal obesity and low FIB-4, suggestive of false positive VCTE.
The Cirrhosis-7 score took the logic of NITs combination further, deriving a multivariable model containing VCTE, controlled attenuation parameter (CAP; Echosens), ELF, platelet count, ALT, international normalised ratio, and BMI to detect MASH cirrhosis with a significant discriminative accuracy, and with sensitivity and specificity both above 80%.9
Finally, several studies cast a shadow over the biomarker optimism, revealing an enormous gap between evidence-based recommendations versus real-word implementation. German laboratory data showed that more than one in five out of 1.4 million patients had metabolic dysfunction rendering them eligible for fibrosis risk stratification.10 Yet, FIB-4 was measured in only 0.11–0.75% of at-risk cohorts, despite its input variables being available for most of the patients. For example, 0.15% of patients with Type 2 diabetes had FIB-4 measured, while ALT, aspartate aminotransferase, and platelet count was available in 61%.
Another study highlighted an even more concerning lack of action following elevated FIB-4: in a 1-year Duke Health pilot study of ELF implementation, endocrinologists saw 1,113 patients with Type 2 diabetes and a FIB-4 ≥2.67.11 Such results should trigger quick referral to hepatology care, but only 25% of those with highly elevated FIB-4 had a subsequent visit at the liver clinic, and a meagre 64 patients received an ELF test to supplement the FIB-4.
CONCLUSION
NITs have moved from diagnostic tests to multi-purpose tools supporting decisions from case finding, risk stratification, treatment selection, and efficacy of intervention, to longitudinal monitoring. The challenge now is implementation, where integration in laboratory information systems, automated reporting in electronic health records, reflex ELF/ADAPT or elastography pathways, and education for non-hepatology physicians and patients on what NIT results mean will be essential to translate the scientific biomarker progress into better access to treatment in real-world clinical care.




