BACKGROUND AND AIMS
Immune checkpoint inhibitors (ICI) targeting programmed cell death-1 (PD-1) and programmed death ligand-1 (PD-L1) have transformed the management of advanced hepatocellular carcinoma (HCC), with combination regimens such as atezolizumab plus bevacizumab now established as preferred first-line options.1 Despite these advances, objective response rates remain variable. This is attributed in part to the uniquely immunosuppressive tumour microenvironment of HCC, characterised by regulatory T cell enrichment, T cell exhaustion, and myeloid-derived suppressor cell infiltration.2 Identifying strategies to enhance ICI efficacy in this setting remains a clinical priority.
Emerging preclinical and clinical evidence suggests that mRNA COVID-19 vaccination may serve as a potent immune adjuvant when administered in proximity to ICI initiation. Grippin et al.3 demonstrated that SARSCoV2 mRNA vaccination triggers a strong Type I interferon (IFN) response that activates innate antigenpresenting cells and enables efficient cluster of differentiation (CD)8⁺ T cell priming against tumour antigens. This occurs through an IFN-dependent process in which dendritic cells acquire and present peptide–major histocompatibility complex Class I complexes, thereby enhancing anti-tumour immunity.3 Concomitant ICI treatment was required for maximal anti-tumour efficacy, particularly in immunologically cold tumours. In large retrospective clinical cohorts, mRNA vaccination near ICI initiation was associated with significantly improved overall survival (OS) in patients with non-small cell lung cancer and melanoma.3 A real-world study in advanced non-small cell lung cancer further confirmed that COVID-19 vaccination enhanced anti-PD-(L)1 immunotherapy efficacy, with vaccinated patients demonstrating superior progression-free survival and OS.4 More broadly, RNA vaccine platforms activate innate and adaptive immune pathways, including pattern recognition receptor signalling and dendritic cell maturation, thereby supporting potent anti-tumour T cell responses.5 A meta-analysis of 10 observational studies encompassing 4,929 patients corroborated these findings, demonstrating improved progression-free survival (pooled hazard ratio [HR]: 0.66; 95% CI: 0.48–0.90) and OS (pooled HR: 0.51; 95% CI: 0.39–0.66) in ICI-treated patients with cancer who received COVID-19 vaccination.6 However, whether this survival benefit extends to HCC had not been specifically investigated.
METHODS
This study evaluated the association between mRNA COVID-19 vaccination and OS among patients with HCC receiving PD-1/PD-L1 inhibitors using the Mayo Clinic Platform (Mayo Clinic, Rochester, Minnesota, USA). A retrospective cohort analysis included patients who received at least one dose of PD-1/PD-L1 inhibitors without liver surgery, stratified by receipt of mRNA COVID-19 vaccine within 6 weeks of immunotherapy initiation. Adjustments were made to include only BMI <30 and exclude patients with diabetes, cardiovascular disease, or heart failure history.
RESULTS
The study results demonstrate that among 4,768 patients (584 vaccinated; 4,184 controls), baseline demographics were comparable. The vaccination group demonstrated significantly improved 5-year OS compared to controls (37.9% versus 23.4%; HR: 0.59; 95% CI: 0.52–0.66; p<0.001; Figure 1). This benefit remained consistent after covariate adjustment and was observed across both female (35.2% versus 22.1%; HR: 0.63; 95% CI: 0.53–0.76; p<0.001) and male subgroups (38.6% versus 22.8%; HR: 0.55; 95% CI: 0.47–0.64; p<0.001), with sustained benefit through 60 months.7
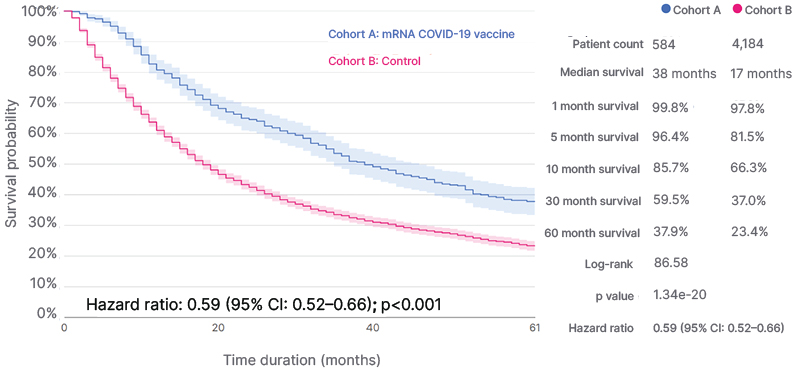
Figure 1: Kaplan–Meier analysis of survival outcomes stratified by vaccination status.
Cumulative survival probability over a 60-month follow-up period for patients in the vaccinated group (blue) compared to the control group (red).
CONCLUSION
These findings extend prior observations in other malignancies to HCC, supporting the hypothesis that vaccine-induced immune priming may synergise with PD-1/PD-L1 inhibition to overcome the immunosuppressive HCC microenvironment.3-5 Importantly, COVID-19 vaccination has been shown to be safe in patients who are ICI treated, with no significant increase in immune-related adverse events.8 Limitations of this study include the retrospective design, potential residual confounding including healthy vaccinee bias, and incomplete follow-up for patients initiating therapy more recently. In conclusion, mRNA COVID-19 vaccination shortly after PD-1/PD-L1 inhibitor initiation may be associated with improved OS in liver cancer, warranting prospective validation and mechanistic investigation.