Abstract
Background: Primary squamous cell carcinoma (SCC) of the gallbladder is a rare, aggressive malignancy with poor prognosis.
Case Presentation: The authors report the case of a 52-year-old woman who presented with cholestatic jaundice and was diagnosed with unresectable gallbladder SCC invading the liver. Despite palliative chemotherapy and haemostatic radiotherapy, her condition deteriorated, and she died 6 months after diagnosis.
Conclusion: This case underscores the aggressive nature and limited treatment options of gallbladder SCC.
Key Points
1. Primary squamous cell carcinoma of the gallbladder is an uncommon and aggressive malignancy, often diagnosed at an advanced, unresectable stage due to its nonspecific clinical and imaging presentation.2. This case highlights the diagnostic challenge of gallbladder squamous cell carcinoma mimicking a hepatic abscess, emphasising the need to consider malignancy when imaging reveals atypical hepatic lesions contiguous with the gallbladder.
3. Early recognition is crucial, as surgical resection remains the only curative option. Palliative chemotherapy and radiotherapy offer limited benefit in unresectable cases, underscoring the poor overall prognosis.
INTRODUCTION
Primary squamous cell carcinoma (SCC) of the gallbladder is a rare histological subtype, accounting for less than 3% of all gallbladder malignancies.1 Unlike the more common adenocarcinomas, gallbladder SCCs are composed entirely of squamous cells without glandular differentiation.2 Their origin remains debated, though chronic inflammation due to gallstones, infections, or anomalous pancreaticobiliary junctions is believed to play a key role in the metaplastic transformation of the epithelium.1,2
Large-scale analyses have shown a clear female predominance, with a median age of onset between 55–65 years.1 In a systematic review by Takahashi et al.,3 and a population-based study of 1,084 cases by Ayabe et al.,1 most patients presented with locally advanced or unresectable disease at diagnosis, reflecting the tumour’s aggressive biological behaviour and poor prognosis.
This tumour type is known for its rapid local invasion into adjacent hepatic and peritoneal tissues and its poor response to systemic therapy.1,3,4 Because of its rarity, there is no standardised treatment, and most data arise from isolated case reports or small case series.1,4
Here, the authors present a case of primary SCC of the gallbladder with hepatic invasion. Beyond its rarity, this case illustrates the diagnostic pitfalls that may occur when initial imaging findings mimic a hepatic abscess. It also emphasises the importance of considering this entity in the differential diagnosis of gallbladder masses with hepatic involvement in order to improve early recognition and management.
CASE PRESENTATION
A 52-year-old woman (gravida two and para two) with no relevant past medical history presented with a 2-month history of cholestatic jaundice and generalised fatigue. Initial abdominal ultrasonography revealed a distended gallbladder with thickened walls, gallstones, and a hypoechoic lesion in the adjacent hepatic parenchyma, initially suggestive of an inflammatory process or hepatic abscess.
Contrast-enhanced CT of the abdomen demonstrated a hypodense lesion in liver segment IV contiguous with the gallbladder wall, associated with pericholecystic inflammation and multiple gallstones. The findings were initially interpreted as a hepatic abscess secondary to acute cholecystitis.
Magnetic resonance cholangiopancreatography subsequently revealed an irregular gallbladder mass invading the hepatic hilum and portal vein, causing intrahepatic biliary dilatation. No distant metastases were detected on chest CT.
Endoscopic sphincterotomy was performed to relieve biliary obstruction. A duodenal biopsy revealed a well-differentiated, keratinising SCC infiltrating the mucosa. Immunohistochemical staining confirmed the squamous differentiation, showing positivity for p63 and cytokeratin (CK)5/6, and negativity for CK7, thereby excluding a poorly differentiated adenocarcinoma. The histopathological features of the tumour are illustrated in Figure 1.
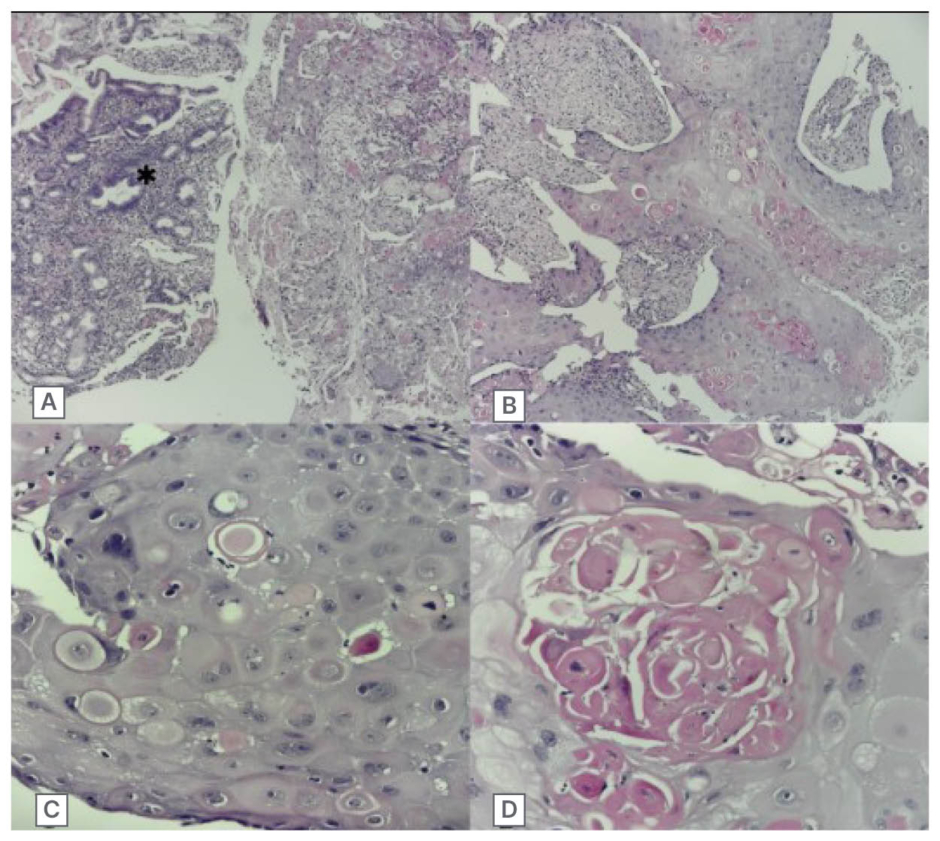
Figure 1: Histologic features of gallbladder squamous cell carcinoma.
Representative micrographs of the tumour showing solid masses infiltrating the duodenal mucosa (A). Tumour cells are large and polygonal with prominent hyperchromatic nuclei and abundant eosinophilic cytoplasm, displaying squamous differentiation including intercellular bridges (B, C). Keratin maturation is evidenced by keratin globules (D) (haematoxylin-eosin stain; magnifications: A, B: ×100; C, D: ×400).
Owing to extensive local invasion, the tumour was deemed unresectable, and palliative chemotherapy with gemcitabine and cisplatin was initiated. During the third chemotherapy cycle, the patient’s performance status declined to WHO Grade 2, with asthenia, vomiting, Grade 1 anorexia, renal impairment, and microcytic hypochromic anaemia.
She was later hospitalised for haematemesis and rectal bleeding. Upper gastrointestinal endoscopy revealed tumour infiltration of the duodenum and biliary tract, confirming disease progression. Haemostatic radiotherapy was delivered, leading to temporary symptomatic relief. The patient’s condition progressively deteriorated, and she died approximately 6 months after diagnosis.
DISCUSSION
SCC of the gallbladder remains a diagnostic and therapeutic challenge due to its rarity, lack of specific symptoms, and aggressive clinical course. While adenocarcinomas account for the vast majority of gallbladder cancers, SCCs exhibit a more infiltrative growth pattern with a stronger propensity for hepatic and vascular invasion.1 These characteristics often make curative resection impossible at the time of diagnosis, as observed in the authors’ patient.
Imaging findings are usually non-specific, and SCC may initially mimic other benign or inflammatory hepatobiliary conditions, such as hepatic abscesses or xanthogranulomatous cholecystitis. In the authors’ case, the lesion was initially interpreted as a hepatic abscess on CT, delaying definitive diagnosis until magnetic resonance cholangiopancreatography and histopathological confirmation were obtained. Similar diagnostic pitfalls have been described in previous reports, emphasising the need for heightened awareness among radiologists and clinicians when evaluating atypical hepatic lesions adjacent to the gallbladder.1
Histopathological examination remains the cornerstone of diagnosis, characterised by keratinisation, intercellular bridges, and keratin pearls. Immunohistochemistry is useful to confirm squamous differentiation (p63+, CK5/6+) and exclude poorly differentiated adenocarcinoma (CK7–).5
Treatment strategies for SCC of the gallbladder are not standardised. Radical surgery offers the only potential for cure, but most cases are diagnosed at an unresectable stage. For inoperable disease, platinum-based chemotherapy (gemcitabine–cisplatin) and radiotherapy may provide palliative benefit, although evidence remains limited and largely extrapolated from biliary tract adenocarcinoma trials.4,6
Several retrospective and population-based studies have confirmed the aggressive nature of SCC of the gallbladder. In a systematic review by Takahashi et al.,3 more than 80% of patients presented with locally advanced or metastatic disease, and median survival rarely exceeded 6 months. Similarly, Ayabe et al.1 analysed 1,084 cases and reported poorer survival outcomes compared to adenocarcinomas, highlighting the urgent need for early detection.
A comparative overview of previously published series and case reports is summarised in Table 1. These studies consistently demonstrate the rarity and aggressiveness of primary SCC of the gallbladder. The majority of patients are diagnosed at an unresectable stage and have dismal outcomes despite surgery or combined treatment modalities.1,3
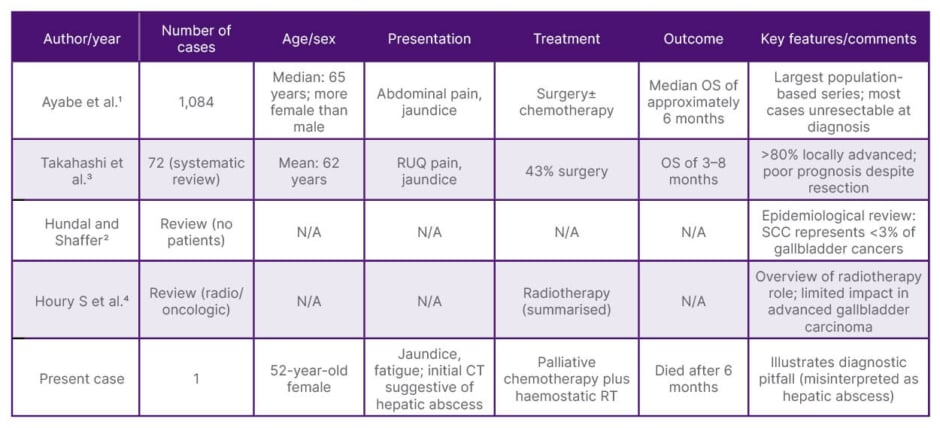
Table 1: Comparative summary of published cases of primary squamous cell carcinoma of the gallbladder.
N/A: not applicable; OS: overall survival; RT: radiotherapy; RUQ: right upper quadrant; SCC: squamous cell carcinoma; vs: versus.
Compared with the authors’ case, which was initially misdiagnosed as a hepatic abscess, most reported cases presented as locally advanced masses with jaundice or abdominal pain. This comparison further underscores the diagnostic challenge and the need for clinical vigilance when interpreting atypical hepatobiliary imaging findings.
The present case contributes to the existing literature by illustrating a locally advanced SCC of the gallbladder initially misdiagnosed as a hepatic abscess, thereby underscoring the diagnostic challenges associated with this rare entity. The educational value of this report lies in raising clinical awareness of this aggressive histologic subtype and promoting early consideration of SCC in the differential diagnosis of gallbladder masses with hepatic invasion.
Further research is warranted to better understand the molecular pathogenesis of SCC of the gallbladder and to identify potential therapeutic targets that could improve prognosis in this devastating disease.
CONCLUSION
Primary SCC of the gallbladder is a rare and aggressive malignancy with poor prognosis and no standardised treatment. This case highlights the importance of maintaining a high index of suspicion when imaging findings mimic benign hepatobiliary conditions such as hepatic abscess. Early recognition is crucial, as surgery remains the only potential curative option.
Beyond its rarity, this report aims to raise clinical awareness of this unusual histologic subtype and to emphasise the need for multidisciplinary collaboration in improving diagnostic accuracy and optimising patient management.






