BACKGROUND
Roux-en-Y gastric bypass and chronic pancreatitis are recognised causes of oxalate nephropathy secondary to fat malabsorption.1 Whipple’s procedure is a lesser-known cause of oxalate nephropathy, and there is only one other reported case to this date.2
CASE PRESENTATION
The authors present the case of a 55-year-old female with a background of Type 2 diabetes, hypertension, and Whipple’s procedure performed 27 years prior for a benign pancreatic cyst.3 The patient presented with a 4-week history of abdominal pain, back pain, and weight loss, and an incidental finding of rapidly declining renal function that had been occurring over a period of 1.5 years. Her creatinine levels had increased from 66 μmol/L in February 2023, to 103 μmol/L in November 2023, to 194 μmol/L at the time of this encounter (Table 1). She denied using nonsteroidal anti-inflammatory drugs. Metformin had been discontinued a month prior by her general practitioner due to impaired renal function.
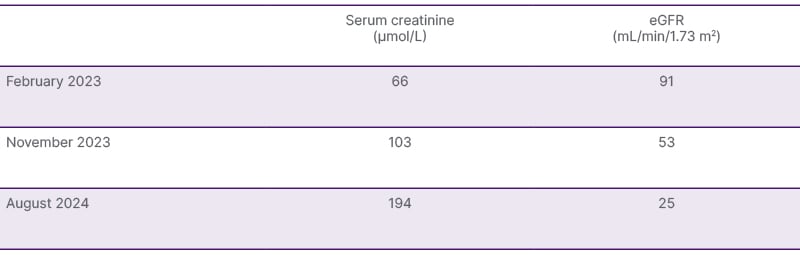
Table 1: Rapid decline in renal function over 1.5 years.
A urine dipstick test was perfomed; the result was unremarkable and revealed no active urinary sediments. The patient’s urine creatinine level was 6.3 mmol/L, her urine albumin was 5.1 mg/L, and the urine albumin to creatinine ratio was 0.8 mg/mmol. Full myeloma and autoimmune panels were negative. A renal biopsy demonstrated multiple intra-tubular oxalate crystals with moderate tubulointerstitial atrophy and glomerular basement membrane thickening suggestive of diabetic glomerulopathy (Figure 1). Total oxalate excretion over 24 hours was 899 μmol. Faecal elastase was <15 μg/g, indicating severe exocrine pancreatic insufficiency. The patient was diagnosed with chronic kidney disease due to secondary oxalate nephropathy, 27 years after her Whipple’s procedure. She remains under follow-up, with the mainstay of treatment being hydration, pancreatic enzyme replacement therapy, and a low oxalate diet.
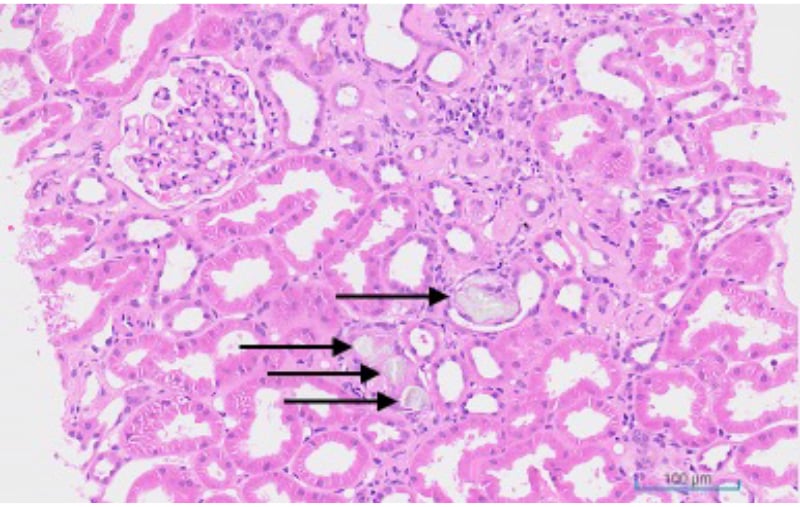
Figure 1: Renal histology.
The sample shows multiple intra-tubular oxalate crystals (black arrows) with adjacent tubular atrophy.
CONCLUSION
Through this unusual case, the authors aim to raise awareness of Whipple’s procedure being a cause of oxalate nephropathy and highlight the possibility of chronic kidney disease occurring decades after the operation.





