Interview Summary
Generalised myasthenia gravis (gMG) is a rare and chronic IgG-mediated autoimmune neuromuscular disease that causes fluctuating and unpredictable muscle weakness. Standard treatment of gMG has traditionally included symptomatic therapy with acetylcholine esterase inhibitors such as pyridostigmine and disease-modifying treatments including steroids, as well as steroid-sparing immunosuppressants and thymectomy. However, it can take months or years for steroid-sparing immunosuppressants or thymectomy to show any clinical benefit, while the side effects of steroids limit their use in practice. With no new therapy options for gMG introduced for decades, a lack of innovation has traditionally meant that a substantial proportion of patients with gMG have been living with uncontrolled disease and a greatly reduced quality of life (QoL). Recently, however, a dramatic change in the treatment landscape has occurred, with a number of new therapies approved for the treatment of gMG, including neonatal Fc receptor (FcRn) blockers and other treatment strategies. These innovative therapies have transformed the lives of patients with gMG, particularly those with highly active disease and otherwise difficult-to-treat myasthenia. During an interview conducted by the European Medical Journal (EMJ), Jan Lünemann, Professor of Neurology and Neuroimmunology at the Department of Neurology, University of Münster, Germany, discussed the use of FcRn blockers, including the human recombinant IgG1-derived Fc fragment, efgartigimod alfa, for the management of gMG from the perspective of his experience in an expert centre in Germany. Lünemann reviewed the past and current treatment landscape for gMG, including a discussion of the outcome measures and treatment goals for the disease. He also described the clinical case of a school teacher with gMG who achieved stable remission and an improved QoL following treatment with efgartigimod alfa, allowing him to continue to teach. Lünemann also offered practical advice on the use of efgartigimod alfa in patients with anti-acetylcholine receptor (AChR) antibody-positive gMG, describing the preferred dosing regimen and identifying potential candidates for this treatment. He closed by summarising some of the benefits of efgartigimod alfa treatment for patients and families affected by gMG.GENERALISED MYASTHENIA GRAVIS (gMG) IS AN IgG-MEDIATED DISEASE
gMG is a rare, chronic, IgG-mediated autoimmune neuromuscular disease caused by antibody-mediated dysfunction of the postsynaptic aspect at the neuromuscular junction.1-8 The characteristic signs of gMG are fluctuating and unpredictable muscle weakness and fatigue,2,4,9 which may lead to a lack of physical energy, poor sleep quality, and a greatly compromised QoL.2 Poor control of symptoms can, in some cases, lead to life-threatening myasthenic crises characterised by respiratory insufficiency or even death.2
RECENT INNOVATIONS IN THE TREATMENT OF GENERALISED MYASTHENIA GRAVIS (gMG): RAPID AND SUSTAINED TREATMENT
Lünemann explained that standard treatment for gMG, which has been unchanged for decades, includes symptomatic treatment with acetylcholinesterase inhibitors such as pyridostigmine, as well as disease-modifying treatments including steroids, steroid-sparing immunosuppressants, and thymectomy.1,2 However, long-term therapy with steroids causes significant side effects,10-12 while clinical efficacy with steroid-sparing immunosuppressants and thymectomy can take months to years to achieve.10,13 The debilitating side effects and notable delay in any signs of improvement have a detrimental effect on patient adherence to medication, further impacting treatment outcomes.12
Lünemann described a change in the treatment landscape over recent years, with the approval of innovative therapies for the treatment of gMG, including FcRn blockers such as efgartigimod alfa.2,14-18 “These new treatment options substantially improve disease management, in particular for those patients with highly active disease and otherwise difficult-to-treat myasthenia,” observed Lünemann. He also explained the benefits of early initiation with innovative treatments, providing a rapid and sustained effect compared with traditional escalation strategies. “In many autoimmune diseases, early and effective disease control is crucial for better long-term outcomes. This is likely true for gMG as well, which is why I strongly advocate for initiating effective medications as early as possible, particularly in patients with high disease activity at onset,” explained Lünemann.
MINIMAL SYMPTOM EXPRESSION (MSE) IS OUR NEW TREATMENT GOAL FOR GENERALISED MYASTHENIA GRAVIS (gMG)
For many years, Lünemann explained, the goal of treatment in gMG was to prevent potentially life-threatening myasthenic crises. However, in 2013, the Myasthenia Gravis Foundation of America (MGFA) defined new treatment goals for myasthenia as a post-intervention status of minimal manifestation, meaning that the patient has no symptoms or functional limitations from myasthenia.10 Similar treatment goals have also been adopted by other national treatment guidelines, including the USA, Germany, and Belgium, for example.2,19,20 “With the approval of the innovative therapies, treatment goals can be achieved for a substantial proportion of patients with myasthenia,” observed Lünemann.
In terms of measuring the outcomes of treatment, Lünemann explained that two standard scales are typically used: the patient-reported MG-Activities of Daily Living (MG-ADL) scale, which covers eight items of daily life, and the more time-consuming physician-reported Quantitative Myasthenia Gravis (QMG) score.3,13 The goal of treatment is to achieve minimal symptom expression (MSE) and sustained remission, defined by a score of 0 or 1 on the MG-ADL scale.21 “The treatment goal for gMG has changed over the past 50 years, and we can now achieve minimal symptom expression for approximately one-third of patients using innovative therapies,” Lünemann commented.
BENEFIT OF NOVEL TREATMENTS SUCH AS EFGARTIGIMOD ALFA EXTENDS BEYOND CLASSICAL MYASTHENIA CLINICAL SCORES: AN ANECDOTAL EXAMPLE OF EVERYDAY STRUGGLES WITH UNCONTROLLED GENERALISED MYASTHENIA GRAVIS (gMG)
Lünemann explained that the age of onset of myasthenia has a bimodal pattern, with one peak at about 30 years of age and another peak around 70 years. Earlier onset disease is around three times more common in females, while later onset is slightly more common in males.1,12 He noted that the patients he sees in his clinical setting in Germany tend to conform to this pattern, but also typically include more difficult-to-treat patients, such as those with a 2–3-year history of poor disease control or myasthenia crises.
Lünemann first gained experience with efgartigimod alfa during the ADAPT clinical trial in patients with gMG.21 However, his extensive experience of using efgartigimod alfa in real-world clinical practice in Germany began with a school teacher with a 4-year history of AChR antibody-positive myasthenia, who greatly feared he would no longer be able to teach because his disease remained uncontrolled, despite multiple therapies. The patient initially started with an MG crisis requiring artificial ventilation, and a subsequent thymectomy was performed 1 year after disease onset. Subsequent treatment with azathioprine was discontinued due to elevated liver enzymes, and the patient was started on methotrexate. After two disease exacerbations managed using intravenous Ig (IVIg) therapy, the patient was treated with steroids at 25 mg/day and referred to Lünemann’s clinic. Lünemann opted for treatment with efgartigimod alfa because the disease was not well controlled and because the patient had responded to IVIg, which has a mechanism of action that partly overlaps with efgartigimod alfa.22 Treatment was initiated at a dose of 10 mg/kg administered intravenously in cycles of once-weekly infusions for 4 weeks, and the patient was regularly monitored, including regular assessment of MG-ADL and QMG scores. Improvement in clinical symptoms was observed, including resolution of double vision after the second infusion of the first cycle, as well as reduced fatigue and a greater ability to carry out everyday activities. The patient’s MG-ADL score reduced from 9 before treatment to 3 after the fourth infusion, and his steroid dose was reduced from 25 mg/day, eventually to complete withdrawal. Once the steroid treatment had been discontinued, the intervals between treatment cycles increased to between 6–9 weeks, and the patient switched from intravenous to subcutaneous administration. Continued treatment with efgartigimod alfa resulted in the patient achieving stable remission, which meant he was able to continue working as a teacher. “The benefit of novel treatments such as efgartigimod alfa extends beyond classical myasthenia clinical scores such as MG-ADL and QMG to tangible improvements in fatigue and quality of life,” noted Lünemann.
PRACTICAL ADVICE FOR USING EFGARTIGIMOD ALFA: HOW TO INITIATE TREATMENT, REDUCE STEROIDS, AND OPTIMISE WEEKS OFF THERAPY
In terms of dosing and redosing, Lünemann observed that efgartigimod alfa may be administered subcutaneously at a fixed dose.16 Alternatively, efgartigimod alfa can be administered intravenously at a dose determined by patient body weight.16 Treatment needs to be administered intravenously once-weekly for 4 weeks, followed by 4 weeks off therapy for the first treatment cycles.16 The aims of this phase of treatment are to determine whether the patient responds to treatment, to achieve a first milestone of stable remission, and to reduce steroid use. From Cycle 2–4 onwards, the time off therapy is adjusted based on clinical evaluation, while the steroid dose is reduced further. After steroids are tapered out, and based on rapid patient monitoring, the intervals between efgartigimod alfa cycles may increase to 6–8 weeks, or even 9 weeks in some patients, according to Lünemann (Figure 1). “We decide dosing on an individual case basis,” he noted.
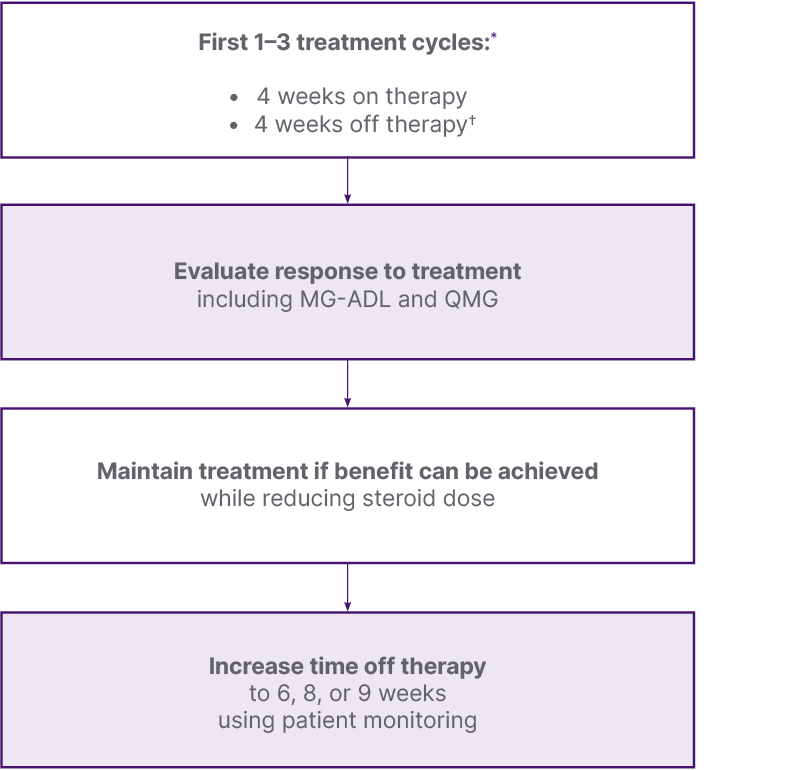
Figure 1: Illustration of the preferred approach to dosing efgartigimod alfa.
*A cycle consists of four once-weekly doses over 22 days
✝Four weeks off starts after the last infusion or injection of the most recent cycle
MG-ADL: Myasthenia Gravis-Activities of Daily Living scale; QMG: Quantitative Myasthenia Gravis score.
A substantial majority of patients respond to efgartigimod alfa treatment, with the ADAPT+ study showing that 81.6% of patients achieved a ≥3-point reduction in MG-ADL by Week 3 of Cycles 1–11 of treatment, and 89% achieved the pre-defined clinically meaningful improvement of ≥2-point reduction in the same timeframe.23,24 However, although treatment response is usually apparent after the second administration of the first cycle,21 it is also important to note that a number of patients may not fully respond to efgartigimod alfa or other novel treatments. Lünemann explained that he usually administers three cycles of efgartigimod alfa to allow for any delay in treatment response; but if there is no significant improvement based on MG-ADL or QMG scores after this time, the patient may be switched to another therapy with a different mode of action.
EFGARTIGIMOD AVAILABLE FOR SELF-INJECTION: SUBCUTANEOUS AND PRE-FILLED SYRINGE (PFS) ADMINISTRATION FORMULATIONS
Initiation of innovative therapies for gMG should always be undertaken in partnership with a specialist centre. When choosing between intravenous and subcutaneous application, patient preference plays a key role. Lünemann noted that subcutaneous application at home is possible after a training phase and offers greater patient autonomy, although some patients prefer to attend the centre on a weekly basis. Lünemann explained that his clinic in Germany has now completely switched to subcutaneous administration, whereby the complete first cycle and the first administration of the second cycle are administered at the centre. The patient is then managed by a neurologist in the community setting and seen at the specialist centre every 3 months. “Unlike treatment for multiple sclerosis,” Lünemann noted, “acceptance of treatment for gMG tends to be high, as patients can often immediately see the benefit of treatment.” Lünemann also observed that the efgartigimod alfa pre-filled syringe, which has recently been approved by the European Medicines Agency (EMA) and is expected to be available in the second quarter of this year,16 would make life easier for patients. He noted that patients sometimes find the preparation needed with other routes of administration to be technically challenging.
Lünemann advised that patients who receive these new therapies should continue to maintain contact with specialist MG centres, with the support of a neurologist in clinical practice. He recommended, based on his own experience in Germany, that the initiation of innovative therapies for gMG should be undertaken in partnership with a specialist centre.
IDENTIFYING SUITABLE CANDIDATES FOR EFGARTIGIMOD ALFA: SHARED DECISION-MAKING WITH THE PATIENT IS ESSENTIAL
Lünemann noted that there are currently no predictive biomarkers available to help identify ideal candidates for efgartigimod alfa treatment. He explained that a process of shared decision-making with the patient is essential prior to treatment initiation, involving educating and empowering the patient, as well as considering patient-centric endpoints, such as convenience (e.g. availability of a pre-filled syringe) and lifestyle (e.g. possibility of self-administration at home or at work), rather than hard clinical study endpoints.
He commented that the decision to use innovative therapies should be made after careful assessment of the balance of benefit-to-risk, taking into account disease activity, treatment risk, and possible alternatives to these treatments. Lünemann explained that he would offer treatment with FcRn to patients who continue to have relevant myasthenic symptoms despite standard of care, including prolonged treatment with long-term steroids or high-dose immunosuppressants, as well as patients who discontinue previous therapy due to side effects, and patients who have been treated repeatedly with IVIg or plasma exchange therapy due to severe myasthenic exacerbations or myasthenic crises. However, he noted that the exact patient type who should be offered FcRn treatment varies slightly between countries according to individual national guidelines.2,19,20,25
Lünemann explained that patients with a history of responding well to plasma exchange therapy or IVIg may also respond to efgartigimod alfa, but this is not always the case. It is also beneficial to treatment success if the patient themselves has a positive attitude towards the treatment. “In general,” Lünemann observed, “once a patient shows a clinical response to therapy, this tends to be maintained for several years.”15
FcRn therapies typically show a positive benefit quickly after initiation, particularly compared with immunosuppressants and thymectomy, providing a window of opportunity to control the condition early in the disease course.14-17 Lünemann suggested that it would also be interesting to study whether this would also provide a rationale for subsequently discontinuing these innovative therapies, or at least lengthening the intervals between treatments (as illustrated by the teacher case study), once the disease state is stable and steroids have been significantly reduced.
SUMMARY
Lünemann concluded by summarising the benefits of innovative treatments such as efgartigimod alfa for patients living with gMG. He noted that these treatments may rapidly help control disease, improve symptoms, eliminate fluctuations, and improve QoL so that many patients are able to lead a normal life without impairment.14-17






