INTRODUCTION
Upper urinary tract urothelial carcinoma (UTUC) is categorised into low-risk (LR) and high-risk (HR) groups based on patient and tumour-specific prognostic factors, according to European Association of Urology (EAU) guidelines.1,2 Traditionally, elective conservative endoscopic treatment (ET) has been reserved for low-risk tumours with a fairly restrictive definition. However, some high-risk patients may benefit from this approach,3,4 as shown by recent changes in the risk-stratification criteria in the 2024 EAU guidelines, where size, multifocality, and hydroureteronephrosis are considered as only weak high-risk factors.2
AIM
The aim of this study was to evaluate the long-term oncological outcomes and renal preservation (RP) rates in patients with HR UTUC undergoing conservative ET, either as an imperative or elective procedure.
MATERIALS AND METHODS
A prospective cohort analysis was conducted on patients with UTUC treated with conservative ET in a single centre from January 2011–January 2024. Exclusion criteria were nodal involvement or metastasis at diagnosis, invasive features on CT urography (uro-CT), tumour stage ≥T1, and histologic variants on initial endoscopic biopsy. Variables analysed included elective versus imperative indication, age, sex, urinary cytology, tumour grade, hydroureteronephrosis, tumour size, location, number, and multifocality, and their association with radical nephroureterectomy (NFU)-free survival, cancer-specific survival (CSS), and overall survival (OS) (Kaplan-Meier curves and Cox regression model).
RESULTS
Out of the 98 patients with UTUC undergoing ET, 71 (72%) met the HR criteria. Among them, treatment was elective in 45 (64%) and imperative in 26 (36%) patients. Eighteen patients (25%) had tumour size ≥2 cm, nine (13%) multifocality (renal and ureteral), 33 (46%) multiple tumours, 36 (51%) hydroureteronephrosis, 12 (17%) high-grade tumours, and 12 (17%) positive cytology.
Over a mean follow-up of 59 months (range: 12–145 months), RP was achieved in 46 patients (65%): 31 (69%) in elective and 15 (58%) in imperative patients. The estimated NFU-free survival was 89% (95% CI: 85–93), 75% (95% CI: 69–81), and 37% (95% CI: 28–46) at 3, 5, and 10 years, respectively, with no statistically significant differences between LR and HR UTUC (Figure 1). No single criteria showed a significant association with RP in bivariate analysis. Multivariate analysis identified multiplicity as the only independent risk factor for NFU (hazard ratio [HR]: 2.1; 95% CI: 1.1–4.3; p=0.03). The CSS at 3, 5, and 10 years was 91% (95% CI: 88–94), 84% (95% CI: 79–89), and 80% (95% CI: 74–86), respectively. No statistically significant differences were found in terms of CSS with the LR group (Figure 1). An OS of 82% (95% CI: 77–87), 69% (95% CI: 63–75), and 49% (95% CI: 39–59) was observed at 3, 5, and 10 years, respectively, with significant differences between LR and HR groups (p=0.04) (Figure 1). Imperative indication was the only independent factor associated with worse OS in HR patients (HR: 4.6; 95% CI: 1.8–11.4). The estimated OS was 52% (95% CI: 42–62) versus 86% (95% CI: 80–92) at 5 years and 35% (95% CI: 25–45) versus 68% (95% CI: 58–78) at 10 years for imperative and elective cases, respectively.
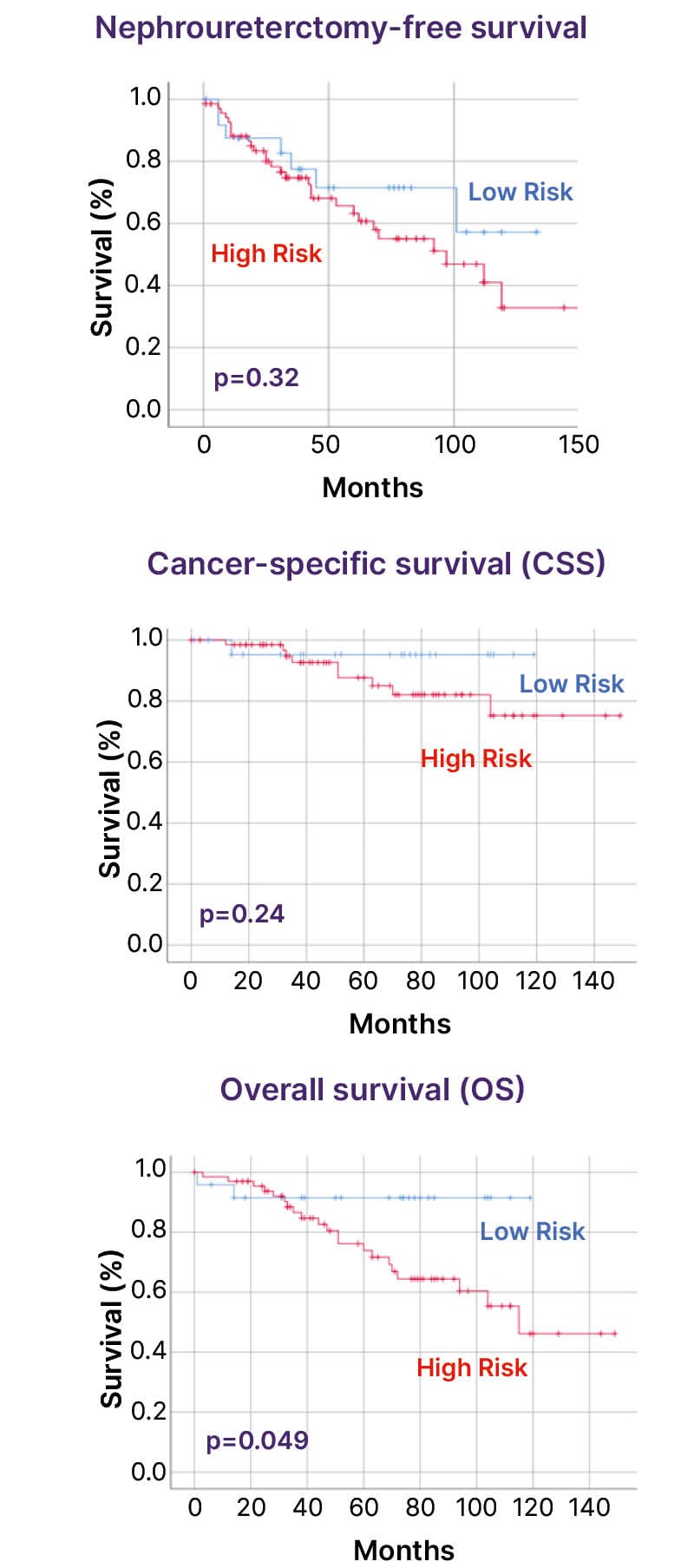
Figure 1: Survival analysis (Kaplan-Meier curves).
CONCLUSION
The authors’ results suggest that conservative ET may be extended to selected HR UTUC cases, including many with factors such as multifocal disease, tumour size ≥2 cm, or hydroureteronephrosis, that, until recently, would have been excluded from this approach according to previous EAU guidelines.





