Abstract
The authors report the case of an 80-year-old Canadian male with a giant bladder stone who declined treatment. A bladder stone is defined as a giant bladder stone when it has a diameter greater than 4 cm or a weight greater than 100 g; they are rare, with less than 100 cases reported in the literature. These stones are even rarer in developed countries like Canada. This pathology usually requires open cystolithotomy for definitive management. To the authors’ knowledge, this is the only reported case of a patient declining treatment, which helps urologists understand the natural history of this condition through a novel growth analysis of the patient’s bladder stone.
Key Points
1. Giant bladder stones are a rare entity, particularly in developed countries such as Canada.2. The authors report a case of an 80-year-old male with a giant bladder stone.
3. This case was novel as the patient declined treatment and the clinicians were able to track the stone growth kinetics.
INTRODUCTION
Bladder stones are solid calculi composed most commonly of magnesium ammonium phosphate, calcium oxalate, calcium phosphate, uric acid, and cystine.1 They encompass approximately 5% of all urological stones and are primarily caused by urinary stasis in the context of benign prostatic hyperplasia (BPH) or neurogenic lower urinary tract dysfunction.2 Bladder stones may cause recurrent urinary tract infections (UTI), haematuria, lower urinary tract symptoms, pelvic pain, and urinary retention.3
A bladder stone is defined as a giant bladder stone (GBS) when it has a diameter greater than 4 cm or a weight greater than 100 g; they are rare, with less than 100 cases reported in the literature.4 These stones are even rarer in developed countries like Canada. This is primarily due to improved access to nutrition at early ages, better fluid intake, increased access to pelvic imaging, and higher socioeconomic status.5 The primary management strategy for GBS is open cystolithotomy.6
The authors report the case of an 80-year-old male with a GBS who declined open cystolithotomy. This patient provided informed consent for his anonymised information to be published in a case report.
CASE PRESENTATION
An 80-year-old healthy White man originally presented with lower abdominal pain and a 3.2 cm stone on abdominal/pelvic CT (Figure 1A). He was not interested in follow-up investigations and he declined treatment for his stone at the time of follow-up with another urologist. He was counselled at that time about the long-term risks of declining further investigations or treatment and did not book any follow-up care.
Three years later, the patient presented to the emergency department with a 24-hour history of suprapubic pain and voiding in small quantities. He complained of mild urgency and frequency, with no other infectious symptoms. He denied gross haematuria.
A new abdominal/pelvic CT scan showed a 6 cm bladder calculus, and mild left kidney pelviectasis (Figure 1B). A 3D CT reconstruction is shown in Figure 2. Creatinine was 138 µmol/L with a baseline of 120 µmol/L. White blood cell count was 10.9×109 /L and haemoglobin was 157 g/L. Urine culture had insignificant growth. Catheter placement with cystoscopy and guidewire failed as the balloon burst shortly after placement. On cystoscopy, the patient had evidence of a moderately obstructing prostate. There were no urethral abnormalities. The urothelium could not be visualised, as the stone was occupying the entire bladder space.
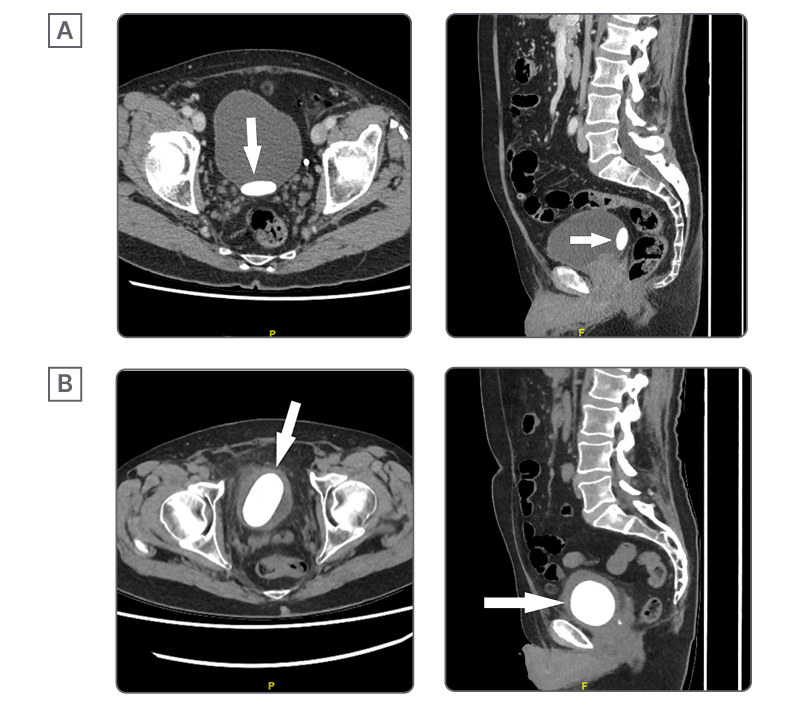
Figure 1: Axial and sagittal CT scans of bladder stone at initial presentation (A) and 32 months after initial presentation (B).

Figure 2: 3D CT reconstruction of bladder stone from 32 months after initial presentation.
During outpatient follow-up, cystolithotomy was discussed with the patient and his family member. Risks of the procedure and estimated risks of not proceeding with treatment were reviewed, including the risk of renal dysfunction, infection or sepsis, pain, and possible bladder rupture. The patient, along with his family member, declined the treatment. He was adamant that he did not want further interventions.
DISCUSSION
Factors that may influence bladder stone formation include BPH, neurogenic bladder, anatomical defects, foreign bodies, urethral strictures, upper tract stones, and recurrent or chronic UTIs.2 Specifically, intravesical prostatic protrusion and reduced urinary flow are independent risk factors in the context of BPH.7 Chronic UTIs are a major contributor, as infected stones may grow rapidly in the presence of urease-producing bacteria.8 In the patient, the most likely aetiology is voiding dysfunction from an enlarged prostate. The patient presented with lower urinary tract symptoms both times; however, he was able to void and had no gross haematuria. He had no reported history of UTIs. While there was potentially a slight decrease in renal function, it is unlikely to be clinically significant given his age.
GBSs are exceedingly rare and mostly seen in tropical or developing countries,9 such as Türkiye, Iran, India, and China; however, even these countries have seen improved rates over the past several years.10 Gadelkareem et al.6 conducted a study on predictors of clinical and surgical characteristics in GBSs in the “stone forming belt” of Africa and Asia. Risk factors for giant stone development included male gender and older age. However, dietary factors may contribute towards GBS formation, even in developed countries. Insufficient fluid intake, high oxalate consumption, low calcium consumption, consumption of mostly carbon 3 plants (e.g., rice, wheat), and high intake of sugar-sweetened beverages have been correlated to the formation of bladder stones. Dietary evaluation is an important component in the assessment of patients with recurrent stone formation, as poor habits and a lack of resources or education can cause stone formation regardless of geography.11
In this case, no intervention was performed at the patient’s request. The literature suggests that an untreated bladder stone may lead to urinary tract damage, recurrent stone formation, bladder damage, urinary retention, infection, and sepsis.2 Further complications for GBS, specifically, have been reported in the literature. Syarif et al.12 reported a case of giant bladder diverticulum associated with a large bladder stone, requiring transurethral bladder neck incision and diverticulectomy with stone extraction. Patients have also been reported to present with renal failure and hydronephrosis in the context of GBS.3,13,14 Furthermore, additional bladder stones may be precipitated by chronic obstruction and mucosal injury associated with such large stones.14 Based on a series of CT images, the progression rate of the patient’s stone was approximately 18 cm3/year (41% per year). The progression rate of bladder stones is not well defined in the literature, and it is not clear if it would be linear. Most case reports outline the time period for which a patient had experienced symptoms, which may vary widely.15,16 Regarding actual growth rate, a recent systematic review and meta-analysis investigated stone growth in asymptomatic renal stones, and calculated a 25% stone growth over an average duration of 43.41 months.17 To the best of the authors’ knowledge, there are no similar articles investigating stone growth rates for bladder stones specifically. The authors found one other report of GBS containing serial imaging, with an initial ultrasound followed by CT imaging later. The rate of stone growth in this case was from 76.0 mm longitudinal and 73.6 mm axial, on ultrasound, to 57.26 mm by 78.25 mm coronal and 79.29 mm by 54.93 mm sagittal, on CT, over the course of 6 months.18
The main options for bladder stone management include spontaneous passage, transurethral cystolithotripsy (TUCL), percutaneous cystolithotomy, and open cystolithotomy. Asymptomatic stones of <1 cm size may be treated conservatively; however, bladder stones are usually symptomatic and require active treatments. The most recent European Association of Urology (EAU) guidelines on bladder stone treatment state TUCL as the intervention of choice for adults and children, where feasible, with a stone-free rate (SFR) of 95–100%. A systematic review and meta-analysis showed no significant difference in SFR between TUCL and percutaneous cystolithotomy. Options for TUCL include a standard rigid cystoscope or a nephroscope, where a nephroscope allows use of large forceps to remove fragments through a 24 Fr sheath, and shorter operative times, where the mean difference is 22.74 minutes (favouring the nephroscope). The main limitation of urethral access is prolonged operative time for very large stones. Percutaneous management is particularly advantageous in cases of very large stones >5 cm or altered urethral anatomy, with an SFR of 90–100%. Tan et al.19 performed a minimally invasive percutaneous procedure using a laparoscopic entrapment bag. In a study of 25 patients with large bladder stones, all patients were stone free and clinically well after this technique. Open cystolithotomy has the highest SFR with 100%, but has a higher risk of complications, including vesicocutaneous fistula formation.20 When endoscopic approaches have higher chances of low SFR, such as in the case of GBS formation, open cystolithotomy may be favoured.6,21 Unique to GBS, cystolithotomy may be more difficult in cases because the bladder stone can adhere to the bladder mucosa. In the study by Gadelkareem et al.,6 it was found that symptom severity, roughness of stone surface, occupation as a farmer, and stone size were correlated with stone adherence to mucosa. The management of bladder outlet obstruction, such as via transurethral resection of the prostate or of the bladder neck, is recommended in patients with multiple or large bladder calculi.22 Pharmacological treatment for bladder stones is limited. Chemical dissolution agents have no established role in the management of GBS given their size, composition, and inability to achieve sustained bladder therapeutic concentrations.23,24 These conservative treatments have had a limited role in the literature for GBS to date.
CONCLUSION
GBSs are a rare entity, particularly in developed countries. The mainstay treatment is open cystolithotomy, though percutaneous surgical approaches have been reported. In this case, 3 years of non-treatment of a GBS resulted in no serious adverse complications, and an estimated growth rate of 18 cm3/year (41% per year).





