INTRODUCTION
Demand for medical imaging is increasing at unprecedented rates1 and many healthcare systems are struggling to cope.2 Reports from the UK NHS suggest that the demand for CT and MRI scans in England is growing by >5% per year.2 The main drivers for these increases are both growth and ageing of the global population.3 In response, workforces have been shown to grow; for example, in the UK, the radiology workforce grew by 6.3% in 2023.4 Although growth was evident, increases in service demand of approximately 11% were still noted for CT and MRI scans in the same year.4 Despite evidence of growth, respondents to a UK Diagnostic Radiography Workforce 2022 Census reported average staff vacancy rates in the region of 12.8%.5 Therefore, the growth rate does not hold pace with current vacancy rates. With rising demands for imaging unlikely to change in the foreseeable future, workforce challenges will likely continue and possibly worsen.6 A traditional response to workforce challenges is a promise to train more healthcare professionals.7 Whilst increased capacity is possible within higher education institutions, the accompanying access to clinical placements is a major global challenge8-10 and is a key limiting factor when seeking to increase the number of diagnostic radiography students admitted for training. Given the significance of the problem, higher education institutions have been asked to consider alternatives to support increases in student training capacity. Such alternatives have included an increased role for clinical simulation11-13 and alternative work-integrated learning, e.g., university-based, industry, and within independent imaging providers. Over recent years, particular growth and interest have been reported using medical simulation. This growth has resulted mainly from recent advancements in profession-specific simulator technologies but also responses to training needs during the COVID-19 pandemic.14 There are now increased options available in terms of 1) the range and quality of simulation possibilities for diagnostic radiography education and 2) the roles for simulation within the curriculum, particularly the potential impact on the requirements for traditional clinical placements. This article, through a review of relevant peer-reviewed literature and policy documents, aims to highlight the range of simulation possibilities within pre-registration diagnostic radiography training and discuss the potential for simulation in terms of substituting or supporting the traditional clinical placement experience.
According to Issenberg and Scalese,15 simulation aims “to imitate real patients, anatomic regions, or clinical tasks or to mimic real-life situations in which healthcare services are delivered.” Within the diagnostic radiography field, different simulators exist (Table 1), including part-task trainers, simulated patients, simulated environments, virtual reality and haptic systems, computer-based simulators, and integrated simulators.17
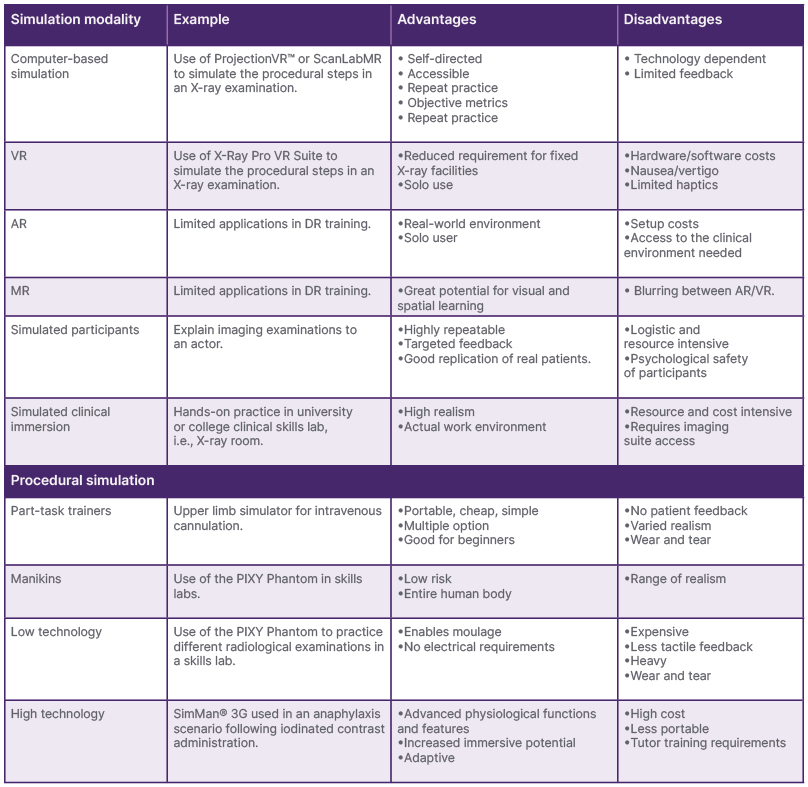
Table 1: Summary of simulation options available within diagnostic radiography.
Adapted from Goodwin and Nestel.16
AR: augmented reality; DR: diagnostic radiography; MR: mixed reality; PIXY Phantom: Southern Scientific, Henfield, UK; ProjectionVR™: Shaderware, Darlington, UK; ScanLabMR: ScanLab, Orlando, Florida, USA; SimMan® 3G: Laerdal Medical, Stavanger, Norway; VR: virtual reality; X-Ray Pro VR Suite: Virtual Medical Coaching Ltd, Christchurch, New Zealand.
It is clear by the vast array of simulation options available that ‘one size does not fit all’. Within any curricula, inclusive pedagogies must be balanced to cater to the full range of learners.18 Currently, the inclusion of simulation in training curricula is governed by multiple factors. These include budgets, simulator availability and quality, student attendance patterns, institutional pedagogical culture, and access to university clinical skills facilities and traditional clinical placements. In many jurisdictions, national regulatory agencies may also place restrictions regarding the use of simulation within radiography education. For example, as part of the UK Nursing and Midwifery Council (NMC) COVID-19 recover programme, up to 600 hours of simulated practice learning experience was permitted.19 By contrast, the UK Royal College of Occupational Therapists (RCOT) provided simulation guidance in the region of 40 hours.20 It is important to note that whilst the quantity of simulation is important, quality remains a significant factor. The quality of simulation technology is likely to also play a significant role in the wider utilisation and adoption. Within radiography education, in the UK, the Society and College of Radiographers (SCoR) has proposed 120 hours of simulation as a recommendation within pre-registration curricula.21
The landscape of simulation within diagnostic radiography education has rapidly evolved; however, detailed guidance, although originally sparse, is now growing. The European Federation of Radiographer Societies (EFRS), in 2021, published a Preliminary Statement on Simulation in Radiography Education.22 Whilst acknowledging many potential advantages for including simulation, this statement also highlighted distinct challenges. These include the need for evidence of the efficacy of using simulation for competency assessments, requirements for educator training in the effective use of simulation, and the need to provide a detailed scope of the requirements for simulation with reference to those technologies focusing specifically on diagnostic radiography. During 2025, the UK SCoR published a simulation model23 and a position statement on the use of simulation in enhancing pre-registration education.21 Outside of radiography education, there are internationally accepted standards for simulation. The Association for Simulated Practice in Healthcare (ASPiH) Standards, published in 2023, focus on elements of theory and evidence-based-practice which are applicable across the broad spectrum of health and care training programmes.24 Other standards and best practice documents have been published, including those from the International Nursing Association for Clinical Simulation and Learning (INACSL),25 Society for Simulation in Healthcare (SSH),26 and the Association of Standardized Patient Educators (ASPE).27 Educators should embrace such documents when designing and implementing simulation into curricula.
Correct selection of a simulation option includes the choice of technology and the role. In many institutions, this includes teaching, learning, and assessments. Decisions regarding the fit of simulation will largely be based on the intended learning outcomes and the previously identified factors, i.e., availability. To alleviate some challenges of increasing the radiographer workforce, one of the dominant questions is to what extent can simulation replace the traditional clinical placement environment? Questions have arisen as to whether radiography training could be delivered with significant utilisation of simulation and without seeking or severely limiting access to the clinical environment. Some commentators might suggest that this could be a step too far.28 Technical glitches and an inability to directly palpate the patient have been highlighted within the literature as potential issues with some simulators.29 Still, some advocate that, given contemporary developments in pedagogies and simulator technologies, simulation could substantially increase its position within training curricula. Much needed guidance on this has arrived from a report delivered in conjunction from the University of Bradford, Society of Radiographers (SOR), and NHS England.21 Within the UK, 120 hours of simulation education is now recommended for pre-registration radiography education. Such developments help foster wider discussions regarding a review of the role of traditional clinical placements and the requirement for a preset quality of ‘clinical’ placement hours. For example, in Ireland, the State regulator, CORU, has reduced the requirement for formal clinical placement hours from 1,200 to 1,000.30,31 Several institutions now advertise in their marketing literature that clinical experience will be a composite of time within clinical departments and university simulation suites, in addition to other pedagogical approaches.32,33
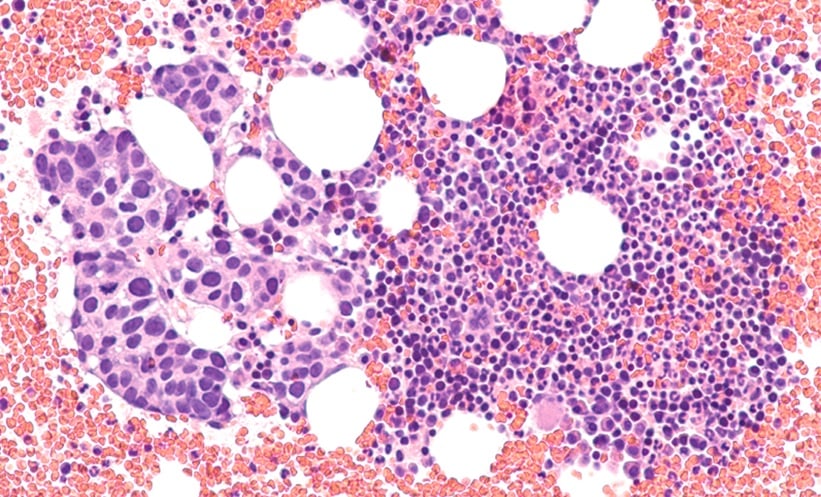
The degree to which the increased use of simulation can expand clinical placement capacity is not currently known. However, in some institutions, a larger student capacity has been possible due to the wider incorporation of simulation support within training curricula.34 In these instances, it is likely that simulation has been introduced to provide essential clinical skills training within the academic environment. Formal robust and objective evaluations of the ability of simulation to achieve the required learning objectives are limited within radiography education. Outside of radiography, studies have shown that simulation can improve clinical skills.35-37 Can simulation be used to train more radiographers? The role of simulation in the aviation industry is not designed to support the training of more pilots. The role of simulation in these instances is to provide experience and evaluations of competencies in rare scenarios, for example, engine failure or extreme adverse weather conditions.38 Even despite the restricted role of simulation in aviation, roles are diversifying and even commercial computer-based flight simulators are considered as ‘flying hours’ by some regulatory authorities.39 Within other areas of healthcare, simulators are a popular training option. For example, virtual reality simulation is reported to play a crucial role in modern surgical training and avoids the need to train ‘on the patient’.40 Similarly, in anaesthesia, the use of simulators in clinical skills training has been an option for over 60 years.41 Likewise, simulation has been used widely in nursing and midwifery education (Figure 1) and has been documented as a valuable strategy for teaching, learning, and evaluating clinical skills.42

Figure 1: An example of a high-fidelity simulator used in nursing and midwifery education.
Note the placement of an intravenous cannula in the right arm, and as such, this mode of simulator could be used in relation to the training of contrast administration during radiological examinations or the management of anaphylaxis.
Bridge and colleagues43 conducted a Delphi study to assess stakeholders’ opinions regarding partially replacing traditional clinical training hours with simulation for the nursing, occupational therapy, orthoptics, physiotherapy, and radiography professions. The consensus opinion from this study was that between 11–30% of clinical training time could be replaced by a simulated placement. While supporting a reduction, stakeholders in the study by Bridge et al.43 did not advocate the complete replacement of clinical placements by simulation. They also did not consider the potential of simulation as a part replacement to current clinical placement rotations. For example, if used with traditional placements, could simulation accelerate the time required to reach designated competencies?
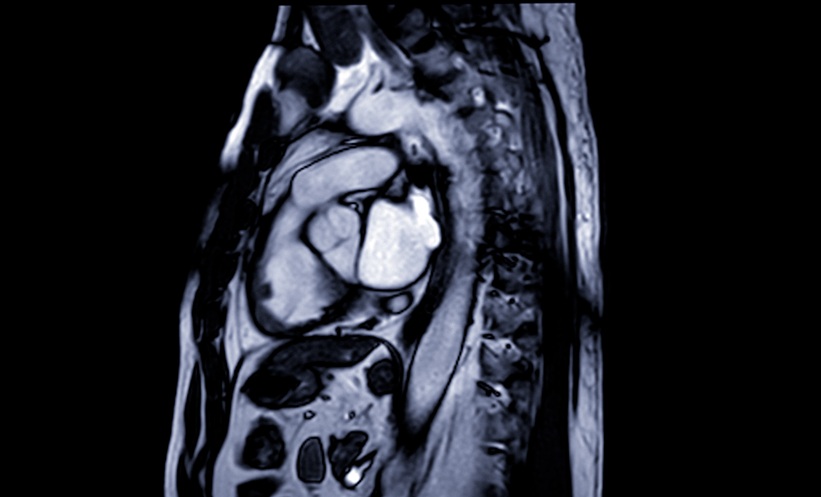
Public perception and acceptance of the role of simulation in pre-registration training is paramount (Figure 2). There is consensus in the literature that the public supports the growth of simulation and favours those demonstrating higher levels of fidelity. Despite this, many would argue that simulation is a supplementary tool and not a direct replacement for experience with patients. By way of an example, patients were more accepting of medical students performing a procedure if they had undertaken training on a simulator, although there were some exceptions, including suturing and intubation tasks.44 A successful health service is based around public confidence in the competencies of the healthcare professionals who work within. Many in wider society might question a bus driver who has solely trained on a simulator or agree to undergo a surgical procedure that has only ever been performed on a simulator. Arguably, traditional clinical placements are not perfect either, and there are frequent media reports about healthcare errors relating to clinical malpractice. A further study, based in surgery, investigated patient and public perceptions of simulation training and reported that both groups were accepting, but improved access and technological developments for simulators were required.45
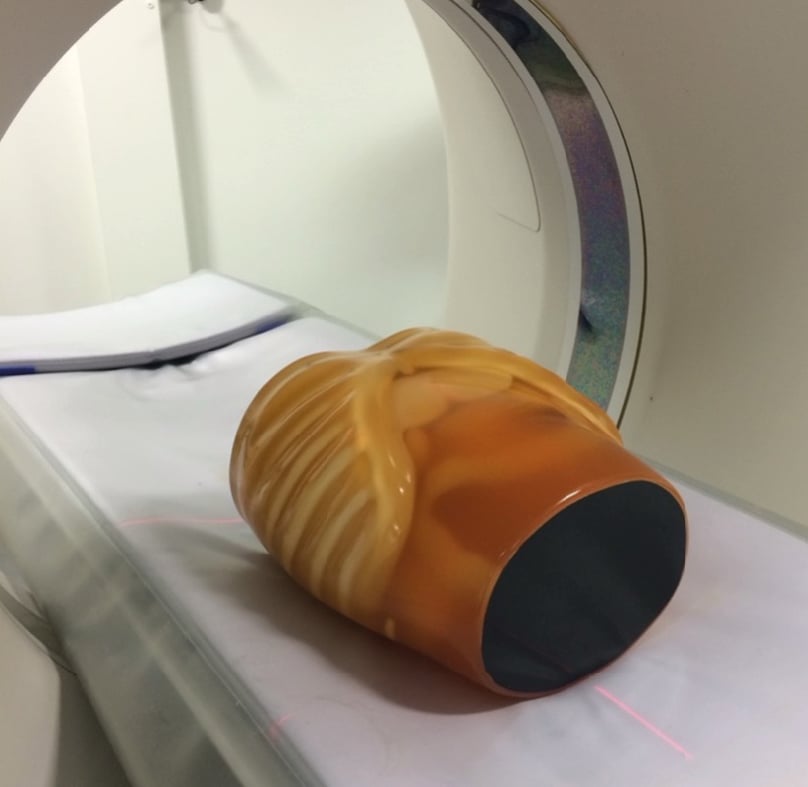
Figure 2: An example of an abdominal anthropomorphic phantom used in CT training.
Note perceptual differences from real patients may reduce realism.
Defining the role for simulation within pre-registration training is multifactorial. Questions arise, such as should the role, quality, and quantity of simulation in pre-registration radiography training be based on robust empirical evidence? One might argue that other areas of radiography training are not subject to such rigor. Also, is it within an educator’s professional role to determine the most appropriate pedagogical approach? Given the rise in availability and complexity of simulation, its use is likely to increase. Managing and harmonising the use of simulation is only likely to be achieved with clear guidance from professional bodies and regulators; fortunately, this is now arriving. If clinical placement provision were an infinite resource, it is likely that discussions regarding simulation and changes to teaching and learning practices would be fewer and far between. This is not the world we live in and demands on healthcare will continue to rise at unprecedented levels. Meeting the challenges of the day will require all hands to the pumps. Achieving this requires inclusion of simulation within all aspects of teaching and learning, but knowing that it is an educational tool to be used alongside others. Developing a stronger evidence base is likely to help with acceptance and procurement but should not preclude the use of simulation in the interim. Professional bodies and regulators must continue to help develop the evidence and guide the inclusion of simulation within health professional training.
CONCLUSION
When considering the current simulation status in diagnostic radiography training, the conclusion is that it is both a substitute and an adjunct. Clinical placement time is decreasing in many jurisdictions but is not being eliminated entirely, possibly because of the increased use of simulation. Simulation is not without frailties, in that annual subscriptions can be expensive and technical support is often required to ensure effective utilisation. Many radiography schools with relatively low cohort sizes may feel that access to a physical skills X-ray room is sufficient. As cohorts grow, the time available for individual students to learn in a physical environment will become less and, possibly, simulation can then play a part. Simulation also provides opportunities to learn about rare events and, thus, is instrumental as an