Abstract
In this case report, the authors present a 67-year-old female with advanced lung adenocarcinoma who developed recurrent haemodynamically significant malignant pericardial effusion. Following multidisciplinary heart team evaluation, percutaneous balloon pericardiotomy was recommended and successfully performed, achieving complete resolution of the effusion with sustained clinical improvement. This case highlights the critical role of interdisciplinary collaboration in guiding optimal therapeutic decision-making and delivering comprehensive palliative care for patients with advanced malignancies.
Key Points
1. Recurrent malignant pericardial effusion is a life-threatening complication in patients with advanced cancer, with high recurrence rates following pericardiocentesis alone.2. Simplifying the procedure as much as possible and limiting the number of implanted stents by using a stepwise provisional strategy remains the recommended strategy for the majority of bifurcation PCI.
3. In this review article, the authors propose the Patient, Lesion, Operator, Technique, and Outcomes (PLOTO) framework to approach bifurcation PCI, which focuses on the five titular components. This model aims to tailor interventions to individual patient needs and help select the most appropriate technique to optimise outcomes.
CASE PRESENTATION
A 67-year-old woman with Stage IV lung adenocarcinoma harbouring an epidermal growth factor receptor-activating mutation and a programmed death-ligand 1 tumour proportion score of 10% was diagnosed with contralateral pulmonary metastases, as well as pleural, pericardial, and osseous involvement. She initially received radiotherapy as part of her treatment regimen.
During subsequent follow-up, she developed a haemodynamically significant pericardial effusion of malignant aetiology. Transthoracic echocardiography revealed signs of cardiac tamponade, including diastolic collapse of the right atrium, a dilated inferior vena cava with less than 50% inspiratory collapse, and exaggerated respiratory variation of mitral inflow velocity (25%). Fluoroscopically-guided therapeutic pericardiocentesis was performed via a subxiphoid approach, yielding approximately 800 mL of haemorrhagic pericardial fluid with transient symptomatic relief. A pigtail catheter was left in situ for 48 hours. Pericardial fluid analysis demonstrated cytology positive for malignant cells with exudative biochemical characteristics; tuberculosis was excluded.
Fourteen days later, the patient reported progressive exertional dyspnoea on reassessment. A repeat transthoracic echocardiogram demonstrated a recurrent pericardial effusion exceeding 500 mL, with echocardiographic evidence of haemodynamic compromise and recurrent cardiac tamponade physiology, including the aforementioned findings. The case was referred to the multidisciplinary heart team, who recommended percutaneous balloon pericardiotomy (PBP) to establish a durable pericardial drainage pathway and mitigate the risk of further recurrence. The primary objective was to optimise the quality of life in a patient with a poor prognosis and a high likelihood of mortality within the first year. Surgical pericardial window creation was considered but was not recommended owing to several factors, including the associated procedural mortality risk and logistical constraints, notably, limited immediate operating theatre availability. This was in contrast to the catheterisation laboratory, which was readily accessible.
The procedure was performed under conscious sedation with anaesthesiology support, via a subxiphoid approach using a 9-Fr introducer sheath. An 18×20 mm balloon catheter was advanced over a guidewire and positioned across the parietal pericardium at the inferolateral aspect. Three sequential balloon inflations were performed under the following parameters: inflation pressure of 3–4 atmospheres and duration of 15 seconds per inflation. Fluoroscopic confirmation of waist disappearance at the pericardial margin was observed during the second inflation, indicating successful disruption of the parietal pericardium. A total of 600 mL of serosanguineous pericardial fluid was aspirated through the sheath. Fluid analysis was not repeated on this occasion, as diagnostic data had already been obtained from the recent pericardiocentesis. The procedure was performed entirely under fluoroscopic guidance, and the team’s expertise enabled its completion without associated complications. A transthoracic echocardiogram performed immediately upon completion of the procedure confirmed the absence of residual pericardial fluid. The patient demonstrated prompt haemodynamic recovery, with resolution of tamponade physiology a nd marked improvement in clinical symptoms (Figure 1).
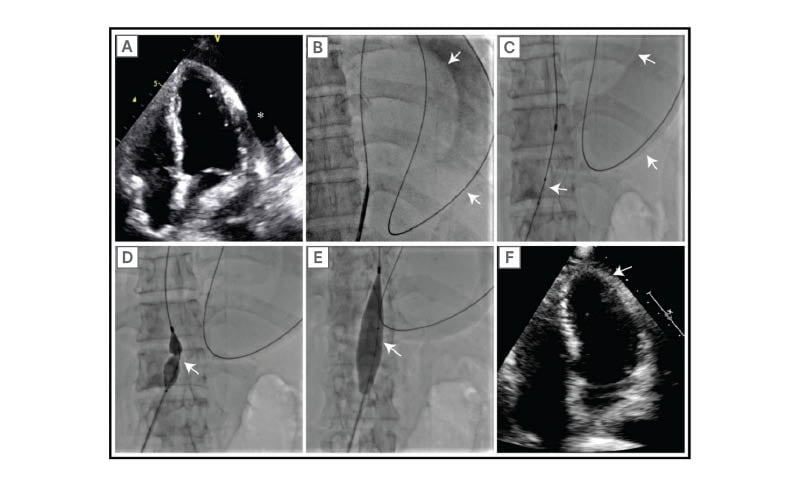
Figure 1: Percutaneous balloon pericardiotomy.
A) Apical four-chamber transthoracic echocardiographic view demonstrating a large, circumferential pericardial effusion with evidence of haemodynamic compromise. B) Subxiphoid approach with advancement of a guidewire into the pericardial space. Contrast injection confirms appropriate positioning, delineating the cardiac silhouette as a discontinuous radiopaque line and the parietal pericardium as a continuous radiopaque line. C) An 18×20 mm balloon catheter was advanced over the guidewire and positioned across the parietal pericardium. D) Initial balloon inflation demonstrating a characteristic waist or indentation at the level of the parietal pericardium, confirming engagement with the pericardial tissue. E) Sequential balloon inflations were performed until the complete disappearance of the pericardial indentation, indicating successful pericardiotomy. F) Post-procedure apical four-chamber transthoracic echocardiographic view demonstrating complete resolution of the pericardial effusion with no residual fluid collection.
The patient reported complete resolution of dyspnoea following the procedure, and serial follow-up echocardiograms demonstrated no recurrence of pericardial effusion over a 6-month period. During her final hospital admission, the patient died as a consequence of her advanced malignancy.
DISCUSSION
This case underscores the critical importance of interdisciplinary collaboration in the palliative management of patients with advanced malignancies complicated by recurrent malignant pericardial effusion despite recent pericardiocentesis. It draws attention to a previously described yet underutilised technique across many catheterisation laboratories worldwide. Through this report, the authors aim to raise awareness amongst a broader range of clinicians and to promote the adoption of this palliative intervention, ultimately improving quality of life and supporting dignified end-of-life care.
PBP is an effective and minimally invasive intervention for recurrent malignant pericardial effusion, capable of significantly alleviating symptom burden and restoring haemodynamic stability, thereby improving quality of life, reducing emergency department admissions, and affording patients more meaningful time with their families. First described by Palacios et al.1 in 1991, this technique remains highly relevant in contemporary clinical practice.2 In their landmark series, approximately 90% of patients who underwent the procedure had an underlying malignancy, and the median survival in this subgroup was only 3.3 months, highlighting the fundamentally palliative nature of the intervention.3
Recurrent pericardial effusion represents a frequently encountered challenge in the management of patients with advanced cancer. Retrospective studies have demonstrated that pericardiocentesis alone in patients with malignant pericardial effusion is associated with recurrence rates as high as 90%, thereby necessitating more definitive drainage strategies such as balloon pericardiotomy.3 Amongst the malignancies most commonly implicated in the development of pericardial effusion, lung and breast carcinomas predominate.4
The current European Society of Cardiology (ESC) guidelines on the management of pericardial diseases recommend PBP as a therapeutic option for patients with recurrent malignant pericardial effusion, designating it as a Class IIb indication.2 In the setting of malignant disease, PBP should be regarded as a primary, less invasive alternative to surgical pericardiectomy or surgical pericardial window creation. Given the markedly limited life expectancy inherent to this patient population, the minimally invasive nature of the procedure confers the additional advantage of substantially reducing hospitalisation duration, thereby preserving valuable time and quality of life during the palliative phase of care.2
Virk et al.5 conducted a systematic review comparing percutaneous and surgical drainage strategies for malignant pericardial effusion and found that PBP offered a favourable balance of low recurrence (approximately 10–14%), with significantly shorter hospitalisation and lower procedural morbidity compared to surgical approaches.5
The authors’ case highlights the pivotal role of interdisciplinary collaboration amongst healthcare professionals in delivering optimal palliative care to patients with advanced malignancies. It further underscores the importance of incorporating both emerging and well-established therapeutic interventions into clinical decision-making, ensuring that treatment strategies are tailored to maximise symptom relief, haemodynamic stability, and overall quality of life in this vulnerable patient population.
PBP is a technically straightforward and safe procedure that has demonstrated efficacy in preventing effusion recurrence in a substantial proportion of patients with haemodynamically significant malignant pericardial effusion.4 Notably, Irazusta et al.4 elected not to incorporate intrapericardial instillation of sclerosing agents in their protocol, reasoning that this approach is poorly suited for this patient population owing to the considerable procedural pain it induces and its potential association with serious complications, including cardiac arrhythmias and constrictive pericarditis.4
The recent series published by Rivero-Santana et al.6 and Kıvrak et al.7 further confirm the safety and efficacy of PBP in contemporary practice, with reported technical success rates exceeding 95% and effusion recurrence rates below 15% during follow-up periods ranging from 30–90 days.6,7
CONCLUSION
PBP represents a safe, effective, and minimally invasive intervention for the management of recurrent malignant pericardial effusion, offering meaningful improvements in both symptom burden and haemodynamic status. Interdisciplinary collaboration and structured longitudinal follow-up remain critical components in optimising the comprehensive care of this patient population. Further prospective studies are warranted to evaluate long-term clinical outcomes, procedural durability, and the broader role of this intervention within the evolving landscape of palliative oncological care.






