Abstract
Atherosclerotic renal artery stenosis is a leading cause of secondary hypertension and is associated with progressive renal dysfunction and clinically significant cardiac syndromes. Although guideline-directed medical therapy remains the first-line approach, revascularisation may provide clinical benefit in carefully selected patients with physiologically significant disease and persistent symptoms despite optimal medical management. Randomised trials, including STAR, ASTRAL, and CORAL, did not demonstrate superiority of renal artery stenting over medical therapy in broadly enrolled populations with predominantly mild-to-moderate disease; however, these neutral findings are likely explained by the inclusion of patients without haemodynamically significant lesions. In contrast, observational data support a role for revascularisation in high-risk phenotypes, including resistant hypertension, ischaemic nephropathy, and cardiac destabilisation syndromes such as recurrent flash pulmonary oedema.
Indications for intervention include persistent hypertension despite treatment with three or more antihypertensive agents, including a diuretic; progressive renal dysfunction attributable to atherosclerotic renal artery stenosis; and cardiac destabilisation syndromes. Diagnostic evaluation typically begins with non-invasive imaging using duplex ultrasound, CT angiography, or magnetic resonance angiography, followed by invasive angiography with physiologic assessment using translesional pressure gradients or renal fractional flow reserve when indicated. Contemporary procedural techniques emphasise minimising aortic manipulation through a no-touch catheter approach, preferential use of radial artery access, and selective use of embolic protection devices. Intravascular ultrasound may optimise stent sizing and expansion, and in-stent restenosis can be managed with balloon angioplasty, repeat stenting, covered stents, or drug-coated balloons.
Complications are uncommon and include access-site bleeding, renal artery dissection, vessel perforation, and contrast-induced nephropathy. Post-procedural care includes duplex ultrasound surveillance and clinical follow-up focused on blood pressure, renal function, and symptom resolution. Renal artery intervention remains an important option in selected patients, with outcomes highly dependent on careful patient selection and contemporary technique.
Key Points
1. An estimated 1.4 billion adults aged 30–79 years worldwide had hypertension in 2024, making it a leading cause of premature death. Over one billion people are currently at risk due to uncontrolled high blood pressure. Atherosclerotic renal artery stenosis is believed to be the underlying cause in approximately 1–5% of all adult hypertensioncases globally.
2. The role of revascularisation has been questioned by trials that largely enrolled broad populations with mild-to-moderate disease, whereas contemporary evidence supports a phenotype- and physiology-guided approach in patients with resistant hypertension, ischaemic nephropathy, or cardiac destabilisation syndromes.
3. Improvements in techniques such as transradial access, embolic protection devices, optimised catheter manipulation, and intravascular ultrasound guidance have contributed to safer and more effective renal artery interventions.
INTRODUCTION
Atherosclerotic involvement of the abdominal aorta and its visceral branches, including the renal artery, is associated with substantial morbidity due to the risk of serious downstream complications. This is strongly linked to traditional cardiovascular risk factors, including advancing age, tobacco use, hypertension, dyslipidaemia, and diabetes. Prevalence increases with age and is highest among individuals with multiple coexisting risk factors.
Atherosclerotic renovascular disease follows a progressive natural history that begins with subclinical vascular changes and may culminate in irreversible parenchymal injury if left untreated. In its early stages, reduced renal perfusion leads to activation of the renin-angiotensin-aldosterone system, often producing renovascular hypertension without significant structural damage. However, with persistent ischaemia, compensatory mechanisms wane, and the kidney undergoes a cascade of deleterious changes, including tubular atrophy, interstitial fibrosis, vascular rarefaction, and mitochondrial dysfunction.1
Studies using blood oxygen level-dependent MRI have demonstrated that renal hypoxia becomes pronounced only after prolonged and severe reductions in blood flow, highlighting a therapeutic window during which revascularisation may be beneficial. Once the kidney crosses this threshold, parenchymal injury may be irreversible despite restoration of blood flow, which likely explains the limited efficacy of revascularisation in late-stage atherosclerotic renovascular disease observed in randomised trials.
Recognising this progression underscores the importance of timely diagnosis and intervention in carefully selected patients.2 Percutaneous renal artery stenting has been shown to be safe and effective for atherosclerotic renal artery stenosis (ARAS); however, several RCTs have not shown superior outcomes when compared to guideline-directed medical therapy (GDMT).3-5 Meta-analyses have shown that, although renal artery stenting achieves very high procedural success rates (>95%), the proportion of patients experiencing meaningful clinical improvement is considerably lower (approximately 70%). This divergence between technical and clinical outcomes is largely attributable to inappropriate patient selection, including intervention on lesions without haemodynamic significance or in patients with primary (essential) hypertension.
It is of paramount importance that the clinician understands clearly which patients are likely to benefit from renal artery revascularisation.6 Careful patient selection, together with meticulous procedural technique, is central to achieving favourable clinical outcomes. The following sections outline the principal indications for renal artery stenting based on the current evidence.
SUPPORTING EVIDENCE BASE
Renovascular Hypertension
Clinical trials have demonstrated that renal artery stenting is both safe and effective, with associated reductions in systolic and diastolic blood pressure. Renal stents have excellent long-term patency rates, with a cumulative primary patency of 79–85% and a secondary patency of 92–98% at 5 years.7,8 Secondary interventions for renal in-stent restenosis (ISR) have higher target lesion revascularisation rates compared to de novo renal stents (21% versus 11%; p=0.003).9 Multiple randomised studies evaluating renal artery stenting failed to demonstrate superiority over medical therapy; however, these trials shared key design features that limit generalisability. Enrollment predominantly included patients with mild-to-moderate angiographic disease, without systematic confirmation of physiologic lesion significance, and excluded individuals with the most severe clinical phenotypes. As a result, a substantial proportion of participants likely had non-flow-limiting disease and limited potential for benefit from revascularisation. This limitation is analogous to the PARACHUTE trial, in which studying low-risk scenarios obscures the benefit of an otherwise effective intervention. These methodological constraints provide a plausible explanation for neutral trial outcomes and underscore the importance of physiology-based patient selection.4,5,10 True resistant hypertension, characterised by persistent systolic blood pressure >160 mmHg and diastolic blood pressure >90 mmHg despite treatment with at least three antihypertensive agents, including a diuretic, at maximally tolerated doses, remains an accepted indication for renal artery revascularisation in the presence of unilateral or bilateral stenosis. Long-term follow-up studies in appropriately selected patients have demonstrated durable blood pressure reduction along with a decreased requirement for antihypertensive medications.11
Ischaemic Nephropathy
Observational studies evaluating renal artery stenting in patients with ischaemic nephropathy consistently demonstrate stabilisation or improvement of renal function when intervention is performed before irreversible parenchymal injury occurs. Improvement is most frequently observed in patients with bilateral disease or a solitary functioning kidney, and in those with rapidly declining renal function prior to intervention. Across cohorts, restoration of renal perfusion is associated with normalisation of contralateral hyperfiltration and preservation of global glomerular filtration, supporting a physiologic basis for benefit in selected patients.12-17
Cardiac Destabilisation Syndromes
ARAS may present with acute or recurrent cardiac destabilisation syndromes, including flash pulmonary oedema, refractory heart failure, and ischaemic cardiac events. These presentations are most commonly observed in patients with bilateral disease or stenosis involving a solitary functioning kidney, where impaired natriuresis leads to volume overload and increased myocardial oxygen demand. In such high-risk phenotypes, renal revascularisation has been associated with meaningful reductions in heart-failure hospitalisations and symptomatic improvement.18-21
DIAGNOSTIC METHODS
Non-Invasive
Renal Doppler ultrasound is commonly used as an initial screening tool for suspected ARAS, while cross-sectional imaging with CT angiography or magnetic resonance angiography may provide complementary anatomic detail when physiologic significance remains uncertain. Each modality has demonstrated high diagnostic accuracy in appropriately selected patients, although advanced renal dysfunction may limit the use of contrast-based imaging techniques.22-24
Invasive
Digital subtraction angiography provides 2D visualisation of the renal arteries, but has limited ability to accurately define lesion severity, as stenoses frequently occur within tortuous and overlapping vascular segments. Expert consensus considers angiographic narrowing greater than 70% to represent severe, haemodynamically significant disease, whereas lesions measuring 50–69% are classified as intermediate and of uncertain physiologic relevance.21 For moderately severe stenoses (50–69%), confirmation of the haemodynamic severity of the ARAS is recommended prior to stenting.25-27
A resting or hyperaemic translesional systolic gradient of ≥20 mmHg, a resting or hyperaemic mean translesional gradient of ≥10 mmHg, or a renal fractional flow reserve (RFFR) ≤0.8 will confirm haemodynamically severe ARAS.25-27 To assess stenosis severity in ARAS, conventional angiography was compared with RFFR and translesional pressure gradients. Angiographic estimates showed poor correlation with both RFFR (r=−0.18; p=0.54) and translesional pressure gradients (r=0.22; p=0.44). In contrast, RFFR demonstrated a strong correlation with translesional pressure measurements (r=0.76; p=0.0016).28
Assessment of the translesional pressure gradient can be performed using a non-obstructive diagnostic catheter or a 0.014-inch pressure wire. Hyperaemic conditions may be achieved with intrarenal administration of papaverine (40 mg) or dopamine delivered as a bolus at 50 µg/kg.28,29 It should be noted that papaverine can precipitate when mixed with heparinised saline solutions commonly used for catheterisation laboratory flushes. In addition, papaverine is no longer widely available in many contemporary catheterisation laboratories.
Although translesional gradients and RFFR are widely used to define haemodynamic significance in renal artery stenosis, these thresholds are largely based on expert consensus. Recent experimental data provide further physiologic support: Drieghe B et al.30 demonstrated in a porcine model that a distal renal arterial pressure/aortic pressure ratio <0.80 is associated with reduced renal perfusion and increased renin secretion.30
More recently, the FAIR randomised trial evaluated a fractional flow reserve (FFR)-guided strategy for renal artery revascularisation compared with conventional angiography-guided decision-making. While overall blood pressure and antihypertensive medication reduction did not differ between strategies, FFR guidance significantly reduced the rate of renal artery stenting. Importantly, clinical benefit from stenting was observed only in patients with haemodynamically significant lesions (FFR <0.80), whereas patients with FFR ≥0.80 did not derive benefit from revascularisation. These findings further support the importance of physiologic lesion assessment to optimise patient selection and avoid unnecessary renal artery interventions.31
INDICATIONS AND CONTRAINDICATIONS
The American College of Cardiology (ACC)/American Heart Association (AHA) guidelines21 and Appropriate Use Criteria (AUC) recommend renal artery stenting in selected patients with haemodynamically significant ARAS, defined as angiographically severe stenosis >70%, or moderate stenosis of 50–69% with physiologic confirmation by a resting or hyperaemic mean translesional gradient ≥10 mmHg or systolic gradient ≥20 mmHg. Clinical scenarios in which revascularisation may be appropriate include recurrent congestive heart failure or sudden-onset ‘flash’ pulmonary oedema, refractory acute coronary syndrome, refractory hypertension despite or intolerant to GDMT, and progressive chronic kidney disease attributable to bilateral renal artery stenosis, stenosis to a solitary functioning kidney, or selected unilateral disease.
There is no indication for the treatment of ARAS in patients who are asymptomatic.25,26 The initial treatment of symptomatic ARAS, as demonstrated in the CORAL trial, is GDMT.4 In patients with ARAS, careful clinical assessment is required to determine whether symptoms are attributable to renal hypoperfusion or whether the stenosis represents an incidental imaging finding. ARAS is frequently identified during abdominal imaging performed for unrelated indications; however, revascularisation is not appropriate in the absence of a relevant clinical syndrome. Similarly, patients with uncontrolled blood pressure who have not yet received maximally tolerated GDMT, including at least three antihypertensive agents with a diuretic, are unlikely to benefit from renal artery stenting. Additional groups with limited expected benefit from revascularisation include patients with advanced chronic kidney disease (Stage III–IV) accompanied by small kidney size (≤7 cm pole-to-pole) and those receiving haemodialysis for 3 months or longer.21,25,26
More recent publications have highlighted the effects of previous RCTs in renal artery stenting. Data from the AHA indicate that renal artery stenting rates in the USA have been decreasing. This decline is attributed to the results of major trials like CORAL, which did not demonstrate a clear benefit of stenting over medical therapy in broad patient populations. Current procedural trends favour treating patients with severe renovascular hypertension, indicating a move towards revascularisation in high-risk populations where the benefits may outweigh the risks.32 A prospective Danish study evaluated high-risk patients with atherosclerotic renovascular disease undergoing renal artery stenting.33 To be eligible for renal artery stenting, patients were required to present with at least one of the following high‐risk clinical syndromes: 1) resistant hypertension with average 24‐hour ambulatory systolic blood pressure ≥130 mmHg (mostly ≥150 mmHg) despite ≥3 antihypertensive drugs, including a diuretic, if tolerated, and each prescribed at optimal doses; 2) rapidly declining kidney function with a reduction in estimated glomerular filtration rate of >5 mL/min per 1.73 m2 per year; or 3) hospital admissions with acute decompensated heart failure (≥2 hospitalisations for heart failure or ≥1 hospitalisations for sudden, ‘flash’ pulmonary oedema) with no obvious explanations such as nonadherence, left ventricular ejection fraction <40%, or valvular heart disease. No interventions were performed if the kidney pole-to-pole length was <7 cm.
Among 96 patients with available 3-month follow-up, the mean 24-hour ambulatory systolic blood pressure declined by 19.6 mmHg (95% CI: 15.4–23.8; p<0.001), accompanied by a 52% reduction in the defined daily dose of antihypertensive therapy (95% CI: 41–62%; p<0.001). Renal function also improved, with an increase in estimated glomerular filtration rate of 7.8 mL/min per 1.73 m² (95% CI: 4.5–11.1; p<0.001). These improvements were sustained at 24 months. Notably, among 17 patients with prior hospitalisations for acute decompensated heart failure, 14 experienced no recurrent episodes following successful revascularisation.33 These findings are summarised in Figure 1.33
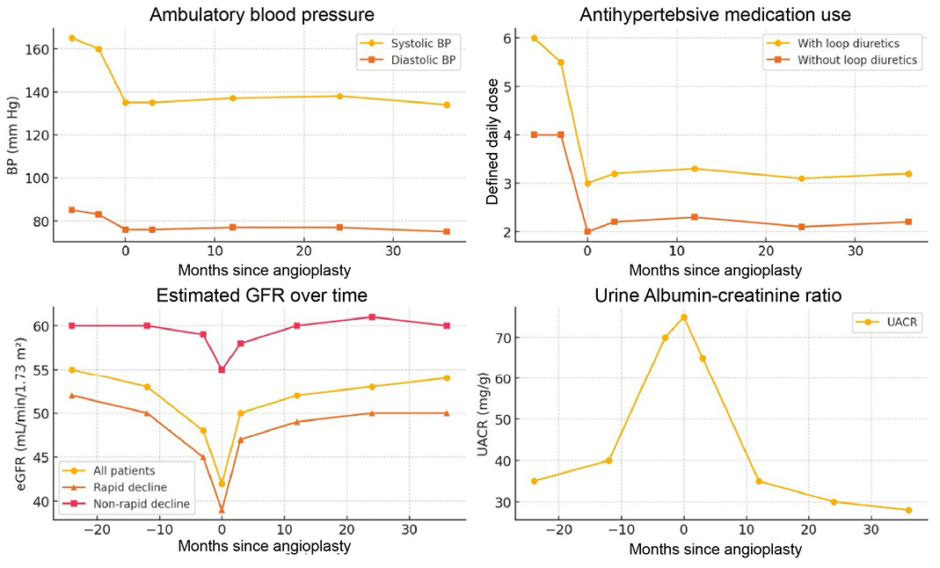
Figure 1: Outcomes after renal artery stenting.
Effects of renal artery stenting in consecutive patients with severe atherosclerotic renal artery stenosis and high-risk clinical presentations, as defined in a Danish national protocol developed in 2015 (DAN-PTRA [NCT02770066]).
Adapted from Reinhard et al.33
BP: blood pressure; eGFR: estimated glomerular filtration rate; GFR: glomerular filtration rate; UACR: urine albumin–creatinine ratio.
PROCEDURAL TECHNIQUE
Pre-procedural Imaging
Before renal artery intervention, a nonselective renal angiogram (aortography) is recommended unless high-quality prior non-invasive imaging, such as CT angiography or magnetic resonance angiography, is available to define aortic and renal arterial anatomy, including the presence of accessory renal arteries.
The Catheter-in-Catheter or No-Touch Techniques
This approach is intended to reduce contact between the guiding catheter and the aortic wall, thereby limiting the risk of renal ostial injury during catheter manipulation. Because ostial atherosclerotic plaque often extends into the adjacent aortic wall, excessive catheter contact can promote distal embolisation. In the no-touch technique, a 0.035-inch J-wire is positioned along the suprarenal aortic wall during renal artery engagement, serving as a buffer that prevents the catheter tip from abrading the aortic surface. After stable engagement is achieved, a 0.014-inch guidewire is then advanced into the renal artery. The catheter-in-catheter technique includes telescoping a smaller diagnostic catheter inside the interventional guiding catheter, allowing engagement with a softer tip catheter and then coaxial engagement of the more aggressive guide.34
Radial Access
Transradial access, using either a 6 Fr sheath or a sheathless 6–7 Fr guiding catheter, is favoured for diagnostic and interventional renal artery procedures, as it reduces access-site bleeding complications, enhances post-procedural patient comfort, and facilitates engagement of the renal artery ostium.
Renal artery interventions performed via radial access require operator familiarity with catheter manipulation, guide selection, and stent delivery, reflecting an inherent learning curve. Use of the left radial artery can offer a more direct path to the renal arteries in some patients. In taller individuals, longer guiding catheters (125–135 cm) and balloon shafts (approximately 150 cm) are often necessary when employing a radial approach. Careful confirmation of stent compatibility with available radial equipment is essential, as delivery of larger-diameter stents may necessitate larger guiding catheters and, in select cases, favour femoral access. Representative angiographic examples of bilateral renal artery stenosis treated with transradial renal artery stenting are shown in Figure 2.
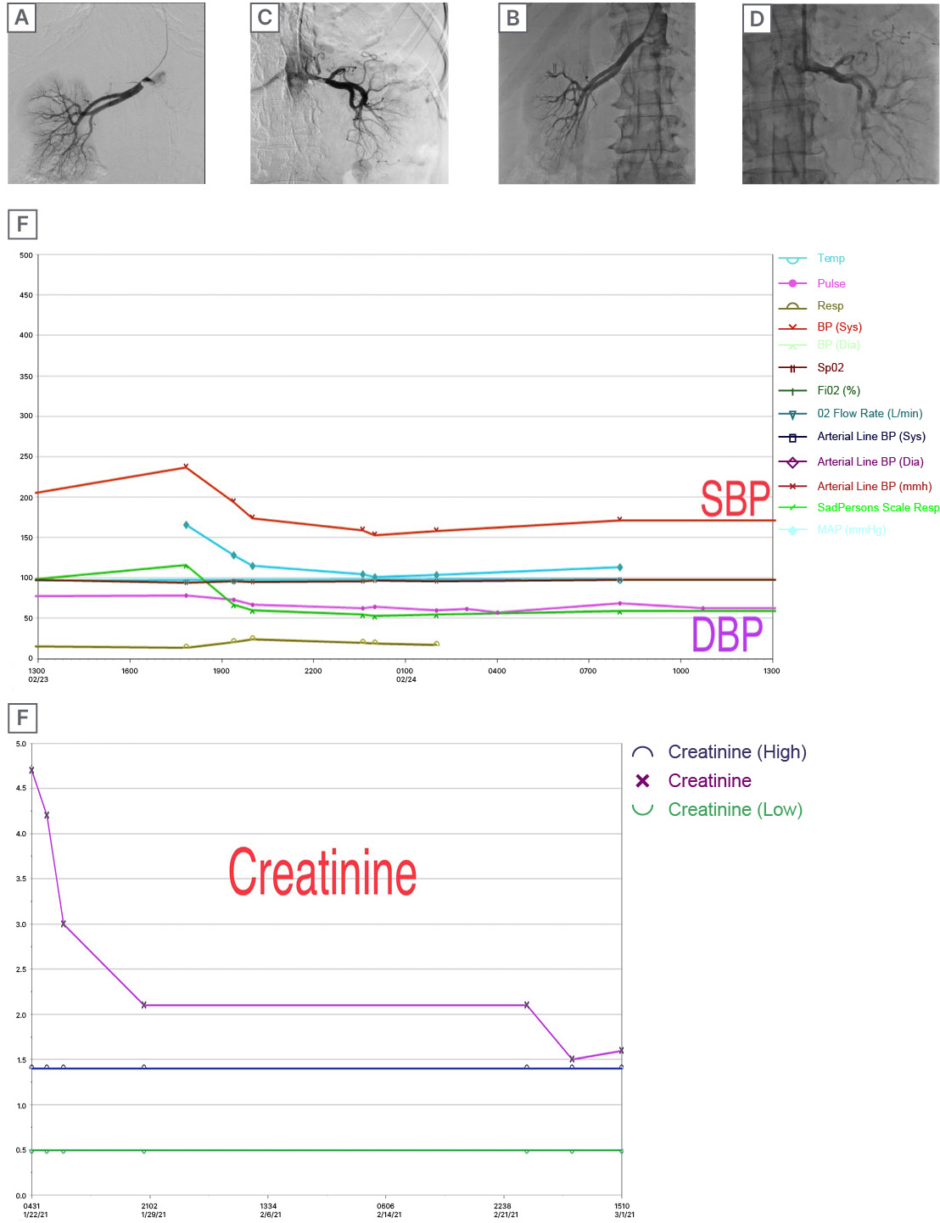
Figure 2: Renal artery stenting examples.
Angiographic examples of bilateral renal artery stenosis before and after transradial renal artery stenting (A–D), with corresponding longitudinal changes in blood pressure (E) and renal function (F) during follow-up.
BP: blood pressure; DBP: diastolic blood pressure; SBP: systolic blood pressure.
Embolic Protection Devices
Atheroembolisation is thought to contribute to postprocedural declines in renal function, which occur in approximately one-quarter of patients following technically successful renal artery stenting. Embolic protection devices may prevent embolic injury during renal stenting and have been shown to be safe.35,36 A small, randomised study (100 patients) looking at patients with chronic kidney disease undergoing renal artery stenting suggested there was preservation of renal function with embolic protection when combined with glycoprotein IIb/IIIa platelet receptor inhibitors.37
Additional evidence is needed to better define the role of embolic protection devices in patients undergoing renal artery stenting across the spectrum of renal function. In the interim, use of embolic protection may be considered in selected high-risk patients with baseline renal impairment to mitigate the risk of atheroembolism-related deterioration in kidney function.
Intravascular Ultrasound-Guided Stent Sizing
Accurate visual estimation of vessel diameter is more challenging in renal arteries, which typically measure between 5–8 mm. Intravascular ultrasound provides a more precise assessment of lesion characteristics, facilitates appropriate stent sizing and expansion, and has been associated with improved clinical outcomes, including better blood pressure control and lower rates of angiographic restenosis. In bare metal renal artery stenting, restenosis is largely influenced by the degree of acute luminal gain, underscoring the importance of safely implanting the largest suitable stent diameter. Although stent undersizing is generally well tolerated, it is associated with a substantially increased risk of restenosis. Careful, selective use of intravascular ultrasound can therefore help operators achieve optimal stent sizing while maintaining procedural safety.38
DES Versus BMS
A prospective trial that compared bare metal stents (BMS) to drug-eluting stents (DES) in ARAS found no difference in the restenosis rate for sirolimus-eluting stents compared to the BMS.39 At 6 months and 1 year, the target lesion revascularisation rate was not different between the two types of stents. Some published data, which did not compare DES to BMS head-to-head, reported outcomes favouring the DES in renal stenting; however, it relied on a hybrid technique of placing a BMS within the DES.40 These findings should be considered exploratory and warrant confirmation in larger, well-designed studies. One important limitation of coronary DES when used in the renal circulation is their relatively low radial strength, a consequence of thinner strut design, which can predispose to stent recoil in the setting of bulky atherosclerotic plaque and external vessel compression. In addition, currently available coronary DES are limited to a maximum diameter of 6 mm, which may be inadequate for larger renal arteries.
ISR Lesions
An optimal strategy for the management of renal artery ISR has not been definitively established, largely because of the absence of head-to-head comparative trials. Available treatment approaches include balloon angioplasty, placement of a DES within a BMS, repeat bare-metal stenting, deployment of covered stents (CS), and the use of vascular brachytherapy.
Repeat renal artery BMS placement demonstrated improved patency compared with balloon angioplasty alone, with a 58% reduction in recurrent ISR (29.4% versus 71.4%, p=0.02).41 Compared with balloon angioplasty alone, repeat BMS implantation was associated with superior secondary patency (p=0.05) and a lower incidence of recurrent ISR (p=0.01). In addition, a non-significant trend towards improved cumulative freedom from target-vessel revascularisation was observed with repeat bare-metal stenting (p=0.08). In a small series of patients having at least their second ISR following BMS, CS had 17% (1/6) ISR at a mean follow-up of 36 months, while coronary DES were free of ISR (0/10).42 There is no established evidence to justify the use of debulking technologies or cutting balloon angioplasty in the management of renal artery ISR. Studies have demonstrated acceptable long-term patency rates and clinical outcomes for CS in renal arteries.43,44 Balloon-expandable CS have been successfully used to treat various indications, including unstable atheromatous lesions and recurrent ISR.43 In a long-term follow-up study, CS effectively excluded renal artery aneurysms while maintaining vessel patency and improving blood pressure control and renal function.44 Notably, CS have been associated with a lower incidence of in-stent stenosis compared to uncovered stents in renal arteries.45
CS in the coronary circulation are linked to higher adverse event rates, such as ISR, reinfarction, and thrombosis, compared to regular stents.46 Despite their critical role in addressing arterial perforations, they pose ongoing risks of thrombosis and restenosis.47 Conversely, CS have shown excellent results in treating visceral artery aneurysms and pseudoaneurysms, with high technical success rates of 96–97% and long-term patency rates up to 88% over a mean follow-up of 32.8 months.48,49 CS appear to be a generally safe and effective option in visceral arteries; however, additional studies are required to better define long-term outcomes and optimal anti-thrombotic strategies.
Drug-coated balloons (DCB) have emerged as a promising therapy for renal artery ISR, showing encouraging efficacy in reducing restenosis rates and maintaining vessel patency, with an acceptable safety profile. Over the last 5–10 years, evidence from clinical practice, including case reports, small observational studies, and analogy to other vascular beds, indicates that DCB angioplasty can achieve high patency in renal ISR lesions that historically often reocclude. Patients treated with DCBs have experienced improvements in blood pressure and stabilisation or improvement of renal function, without the need for additional stents. When comparing treatment modalities, DCBs offer a unique advantage of combining the antirestenotic efficacy of local drug delivery (seen with DES) with the avoidance of additional metal layers (as with plain angioplasty). Early data suggest DCB outcomes are at least on par with repeat stenting, and likely superior to plain balloon angioplasty in terms of preventing recurrent stenosis.50,51
COMPLICATIONS AND THEIR MANAGEMENT
Vascular Access
Access-site complications represent the most frequent adverse events during renal artery interventions and are predominantly associated with femoral access, including haematoma, pseudoaneurysm formation, arteriovenous fistula, and retroperitoneal haemorrhage. These complications are substantially reduced when a transradial approach is employed. Management strategies for femoral access complications may include CS placement, thrombin injection for pseudoaneurysms, and surgical vascular repair when indicated.52,53
Vessel Rupture and Dissections
Severe or catastrophic complications associated with renal artery stenting are rare. The overall incidence of major complications with renal artery stenting is about 2%.53 Significant renal artery dissection most commonly results from subintimal guidewire passage, excessive catheter manipulation, predilation beyond vessel tolerance, stent oversizing, or aggressive balloon expansion. Use of hydrophilic guidewires is generally discouraged because of the increased risk of vessel perforation.
Maintaining guidewire access across the lesion is essential during the management of renal artery complications. When wire access is preserved, a dissection flap can often be treated with prolonged balloon inflation or by deploying an additional stent. In cases of acute arterial thrombosis, local administration of thrombolytic therapy may be effective; however, restoration of luminal patency is required for fibrinolysis to be successful.
If vessel perforation occurs, initial management should include reversal of anticoagulation and sustained balloon inflation to achieve haemostasis. CS may be used to treat intraprocedural complications, such as perforation or vessel rupture. In rare situations where bleeding cannot be adequately controlled, surgical intervention, including nephrectomy, may be necessary.
Follow-Up and Surveillance
The current AUC recommendations for duplex ultrasound (DUS) follow-up after renal intervention are that it is ‘appropriate’ to perform a post-stent baseline study within 30 days of the procedure.54 It may be appropriate to perform additional DUS studies at 6 months and/or 9 months. It is ‘appropriate’ to perform a follow-up DUS at 12 months and annually thereafter.
When duplex imaging is performed after renal stent placement, it is important to make adjustments to the velocity parameters post-stenting compared with a native vessel, as decreased compliance due to the stent will result in higher velocities.22 Accordingly, performing a post-procedural DUS is reasonable to establish a new baseline peak systolic velocity. If surveillance imaging identifies anatomic ISR, reintervention should be considered only when clinical criteria are met, such as persistent resistant hypertension despite GDMT, progressive chronic kidney disease, or the development of a cardiac destabilisation syndrome. In the absence of these features, many patients with stable ISR can be safely managed with continued medical therapy and serial duplex surveillance over prolonged follow-up.
FUTURE DIRECTIONS
Despite decades of investigation, optimal patient selection and timing for renal artery revascularisation remain unresolved. Emerging data support a phenotype-driven approach, yet no validated algorithm exists to reliably identify patients most likely to benefit from intervention. Future research should focus on developing predictive tools that integrate clinical, imaging, and biochemical markers. Prospective trials targeting high-risk phenotypes, such as patients with recurrent flash pulmonary oedema, rapidly declining renal function, or resistant hypertension verified by ambulatory blood pressure monitoring, are urgently needed. Additionally, the role of novel therapies (e.g., DCBs, CS) and adjunctive therapies (e.g., anti-fibrotic agents) in improving post-revascularisation outcomes warrants systematic evaluation. Finally, given the heterogeneity in disease course and response, the creation of multicentre registries and the application of machine learning to large clinical datasets may help define more nuanced, individualised treatment pathways.
SUMMARY
Haemodynamically significant ARAS arises from flow-limiting narrowing of the renal arteries and is associated with clinically important sequelae, including resistant hypertension, ischaemic nephropathy, and cardiac destabilisation syndromes such as flash pulmonary oedema and acute coronary events. Contemporary evidence indicates that the clinical benefit of renal artery revascularisation is highly dependent on careful patient selection, with the greatest benefit observed in patients with physiologically severe disease and persistent clinical syndromes despite maximally tolerated GDMT. The heterogeneous outcomes reported in prior randomised trials largely reflect enrollment of patients without haemodynamically significant lesions, underscoring the importance of integrating physiologic assessment into decision-making.
When revascularisation is indicated, a transradial approach is preferred to reduce access-related complications and facilitate catheter engagement. Adjunctive use of intravascular ultrasound can optimise stent sizing and expansion, while selective use of embolic protection devices may mitigate atheroembolic risk in patients who are at high-risk. Post-procedural management should emphasise longitudinal surveillance with clinical assessment, laboratory evaluation of renal function, and DUS imaging to monitor for ISR. When applied judiciously and with contemporary technique, renal artery intervention remains an important therapeutic option for carefully selected patients with clinically significant ARAS (Figure 3).
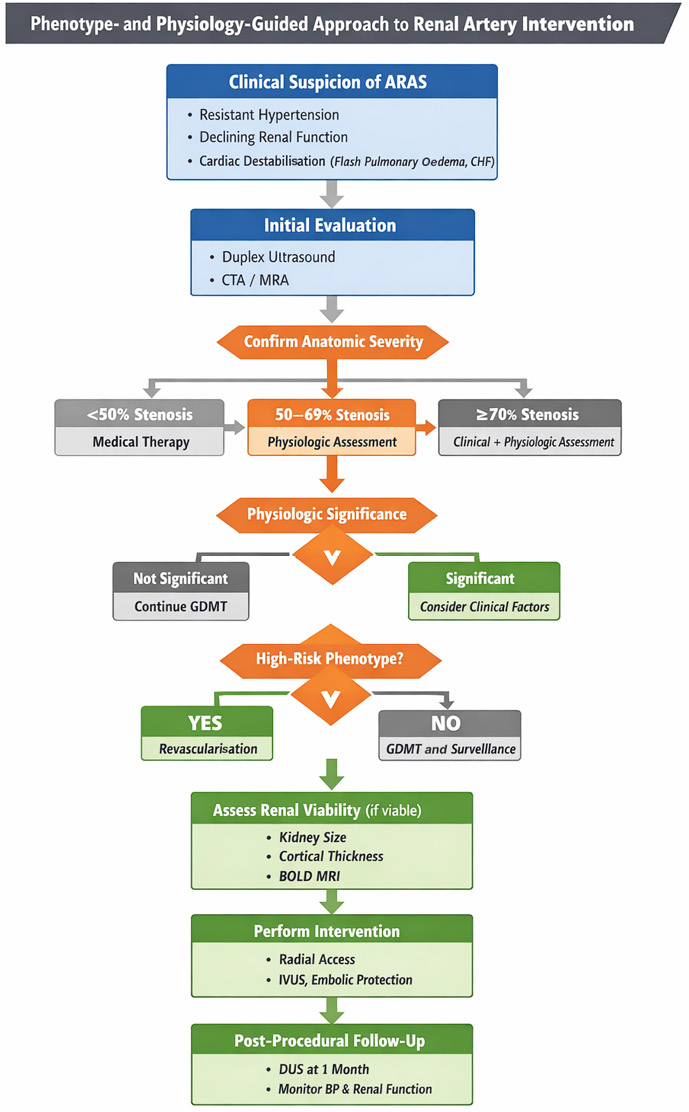
Figure 3: Phenotype and physiology-guided approach to renal artery intervention.
This algorithm outlines a stepwise approach to the evaluation and management of ARAS. Clinical suspicion is based on resistant hypertension, declining renal function, or cardiac destabilisation syndromes. Initial evaluation includes non-invasive imaging with DUS, CTA, or MRA, followed by confirmation of anatomic severity. Lesions <50% are managed medically, while intermediate stenoses (50–69%) require physiologic assessment, and severe stenoses (≥70%) warrant combined clinical and physiologic evaluation. Revascularisation is considered only in patients with haemodynamically significant disease and a high-risk clinical phenotype. Additional assessment of renal viability may guide decision-making. When intervention is pursued, contemporary techniques such as radial access, IVUS guidance, and embolic protection may be employed. Post-procedural follow-up includes DUS surveillance and clinical monitoring of BP and renal function.
ARAS: atherosclerotic renal artery stenosis; BOLD MRI: blood oxygen level-dependent MRI; BP: blood pressure; CTA: CT angiography; DUS: duplex ultrasonography; GDMT: guideline-directed medical therapy; IVUS: intravascular ultrasound; MRA: magnetic resonance angiography.





