Abstract
Herpes simplex virus Type 1 (HSV-1) encephalitis is the most common cause of sporadic fatal encephalitis worldwide, associated with significant morbidity and mortality despite antiviral therapy. While atypical presentations, such as urinary and bowel incontinence, have been documented, their prevalence remains uncertain. MRI is the modality of choice, typically revealing asymmetrical hyperintensities in the mesiotemporal and orbitofrontal lobes, and insular cortex on T2-weighted sequences.
The authors report a case of HSV-1 encephalitis characterised by prodromal symptoms, followed by urinary incontinence, impaired working memory, reduced verbal output, and hypoemotionality, features commonly associated with frontal lobe syndromes. HSV-1 was detected in cerebrospinal fluid analysis, and MRI demonstrated hyperintensity in the cingulate gyrus and insular cortex with leptomeningeal enhancement, correlating with the patient’s clinical presentation. The patient achieved full recovery following a 21-day course of intravenous acyclovir.
Unlike the classic temporal lobe involvement seen in HSV encephalitis, frontal lobe lesions may present with symptoms reflective of frontal lobe dysfunction, posing diagnostic challenges and potentially delaying treatment. MRI findings may aid in identifying frontal lobe involvement in such cases. Therefore, early empirical antiviral therapy should be initiated while awaiting definitive test results to minimise neurological sequelae and improve patient outcomes.
Key Points
1. Herpes simplex virus (HSV) encephalitis typically affects the temporal lobes; however, it may present as a frontal lobe syndrome. Symptoms related to frontal lobe dysfunction pose diagnostic challenges and potentially lead to delays in treatment. Early diagnosis with prompt initiation of antiviral therapy may reverse symptoms related to frontal lobe dysfunction.
2. In this case report, the authors present a case of HSV Type 1 encephalitis with atypical presentation, such as urinary incontinence and executive dysfunction. MRI features correlate with frontal lobe involvement. The diagnosis was confirmed with HSV Type 1 detected in cerebrospinal fluid analysis.
3. Clinicians should consider HSV encephalitis in patients with frontal lobe dysfunction.
INTRODUCTION
Herpes simplex virus (HSV) encephalitis is the most common cause of sporadic fatal encephalitis worldwide, primarily caused by HSV Type 1 (HSV-1) and, less frequently, HSV Type 2. The majority of cases are attributed to HSV-1. HSV encephalitis affects individuals across all age groups, with an estimated annual global incidence of 2–4 cases per million population. Without appropriate treatment, the mortality rate approaches 70%, while antiviral therapy reduces mortality to approximately 30%.1
The common clinical manifestations include confusion (81%), fever (76%), headache (70%), abnormal behaviour (66%), speech disturbances (57%), and seizures (55%).2 Atypical presentations, such as urinary and bowel incontinence, have been reported, although their prevalence remains uncertain. MRI is the preferred diagnostic modality, typically revealing asymmetrical hyperintensities in the mesiotemporal and orbitofrontal lobes, and insular cortex on T2-weighted sequences.3
This case report underscores the potential involvement of the frontal lobe in HSV encephalitis, which may contribute to urinary incontinence due to its role in urinary control.
CASE REPORT
The authors present the case of a 65-year-old female who was admitted with a 2-day history of abnormal behaviour, bilateral lower limb weakness, and urinary incontinence. Further history revealed difficulties in memory and responsiveness during conversations with family members. She exhibited word-finding difficulties, reduced motivation, and a lack of drive and interest during interactions. Additionally, she experienced episodes of urinary incontinence and reduced bowel output. A prodromal phase, including low-grade fever, malaise, headache, and nausea, had occurred 1 week before symptom onset. Premorbidly, the patient was well-spoken, active, and independent in her daily activities. Her past medical history included well-controlled diabetes, hypertension, and hyperlipidaemia.
On presentation, her vital signs were stable: blood pressure of 136/74 mmHg, heart rate of 84 bpm, respiratory rate of 18 breaths per minute, temperature of 37.6 °C, oxygen saturation of 97% on room air, and capillary blood glucose of 7.3 mmol/L. Clinically, she appeared distracted but remained oriented to time, place, and person. Speech assessment revealed slow and halting responses with word-finding difficulties, suggestive of transcortical motor aphasia. Additionally, she exhibited apathy and abulia. Her Mini-Mental State Examination (MMSE) score was 16/30.
Neurological examination revealed increased muscle tone in the lower extremities. Motor strength was reduced, with a power of 3/5 on the right side and 4/5 on the left. Deep tendon reflexes were exaggerated bilaterally, with no clonus. Babinski’s reflex was negative. Sensory examination identified a loss of vibration and proprioception in the right lower limb, while soft touch and pinprick sensation remained intact. Rectal examination demonstrated reduced voluntary anal contraction and decreased deep anal sensation. A Foley catheter was inserted for continuous bladder drainage due to a distended bladder at presentation.
Initial laboratory investigations, including complete blood count, renal profile, liver function tests, and electrolytes, were within normal limits. C-reactive protein was mildly elevated at 22.1 mg/L (reference range: <5 mg/L). Contrast-enhanced CT of the head showed no significant abnormalities. EEG demonstrated mild theta slowing in the frontal region, indicative of mild-to-moderate cortical dysfunction. Subsequent MRI revealed marked hyperintensities in the bilateral cingulate gyrus, suggestive of inflammatory changes, along with leptomeningeal enhancement (Figures 1 and 2).
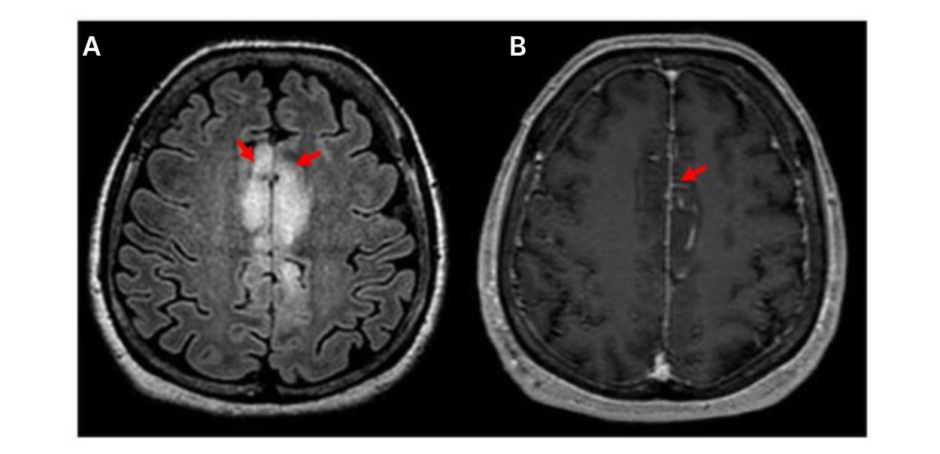
Figure 1: A) FLAIR axial shows marked hyperintensities suggestive of inflammatory changes at bilateral cingulate gyrus; and B) T1 MPRAGE post contrast axial demonstrates associated mild leptomeningeal enhancement.
FLAIR: fluid-attenuated inversion recovery; MPRAGE: magnetization-prepared rapid gradient-echo.
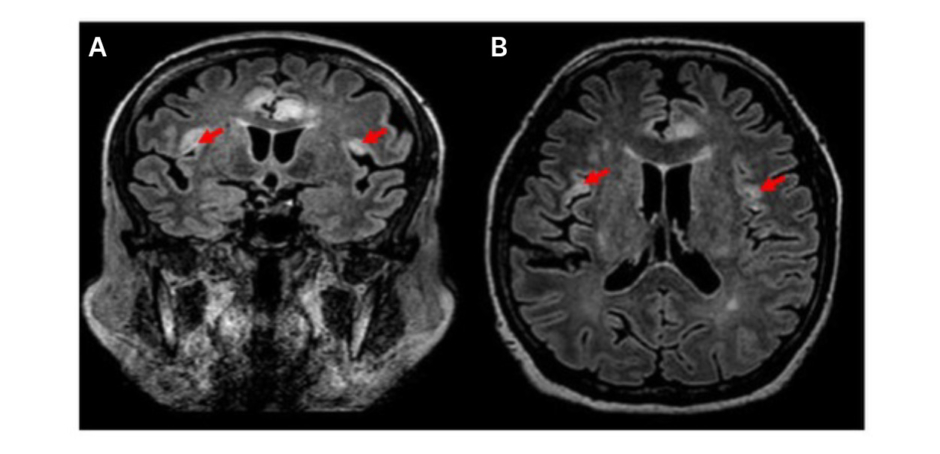
Figure 2: A) FLAIR coronal; and B) FLAIR axial shows lesser inflammatory changes at bilateral insular cortices, with no obvious changes in the mesial temporal lobe.
A lumbar puncture was performed, revealing an elevated opening pressure of 41 mmHg. Cerebrospinal fluid (CSF) analysis showed elevated protein levels (0.7 g/L; reference range: <0.45 g/L), normal glucose (3.3 mmol/L; reference range: 2.5–5 mmol/L), and negative Gram stain and culture. HSV-1 was detected in the CSF. Screening for hepatitis B surface antigen, hepatitis C virus antibodies, and HIV antibodies was negative. Autoimmune encephalitis panel (anti-NMDAR, anti-AMPA1/2, anti-CASPR2, anti-LGI1, anti-DPPX, anti-GABA B) and paraneoplastic antigen antibodies (amphiphysin, CV2, PNMA2, Ri, Yo, Hu, SOX1, recoverin, titin) were also negative.
The patient was treated with intravenous acyclovir for 21 days. By Day 16 of hospitalisation, she achieved successful trial micturition, indicating recovery of bladder function. Her MMSE score improved to 30/30 prior to discharge. She was ultimately discharged in good condition with full neurological recovery.
FOLLOW-UP AND OUTCOMES
At the 3-month assessment, the patient had fully resumed all her premorbid activities of daily living. Complete recovery of speech, behaviour, and executive function was observed. Her cognitive assessment was normal, with an MMSE of 30/30. Neurological examination was unremarkable. A repeat urodynamic study at 3 months confirmed restoration of normal bladder function. Figure 3 shows the timeline of events.
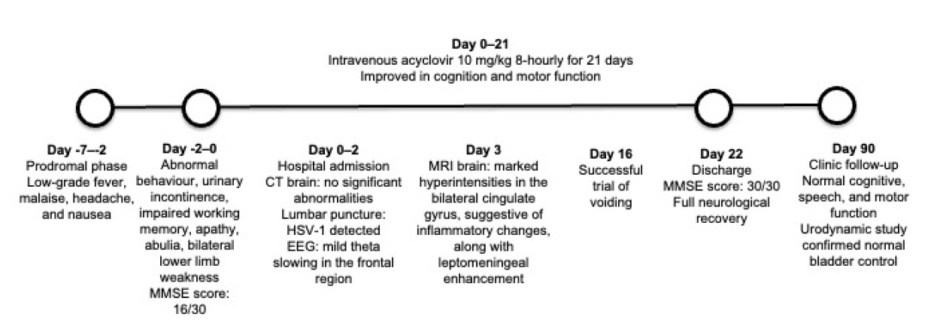
Figure 3: Timeline.
HSV-1: herpes simplex virus Type 1; MMSE: Mini-Mental State Examination
DISCUSSION
Herpes simplex encephalitis (HSE) primarily affects the temporal lobes, which are responsible for memory and speech.1 However, in rare cases, it can also impact the frontal lobes, which regulate behaviour, emotions, and, notably, bladder control, particularly within the medial aspect of the prefrontal cortex.4-6
HSV gains entry via the oral mucosa, followed by retrograde transmission along the trigeminal or olfactory nerve pathways. Reactivation of latent infection via the trigeminal route is classically associated with temporal lobe presentation. The olfactory pathway facilitates virus transmission to the frontal and mesiotemporal lobes, contributing to frontal lobe symptoms.
In this case, the patient presented with a subacute history of frontal lobe syndrome and executive dysfunction secondary to HSE. Damage to the anterior cingulate or the medial frontal circuit is known to result in a spectrum of impairments related to motivation and volitional behaviour.7 This patient exhibited abulia, apathy, and transcortical motor aphasia.8,9
Executive functioning encompasses a broad range of higher-order cognitive abilities, including planning, goal-directed behaviour, and attentional control. These skills, which are essential for managing daily tasks such as problem-solving, adapting to new situations, and decision-making, are primarily governed by the prefrontal cortex.7
The frontal lobe, particularly the anterior cingulate gyrus and inferior frontal gyrus, plays a critical role in the higher-level regulation of bladder function, including the voluntary decision to urinate. Damage to these areas can result in incontinence.10
The presence of frontal lobe dysfunction and behavioural abnormalities may mimic several alternative diagnoses, including autoimmune encephalitis, stroke, and primary psychiatric disorders. Autoimmune encephalitis, particularly anti-N-methyl-D-aspartate (NMDA) receptor encephalitis, is typically confirmed by the presence of IgG anti-GluN1 antibodies. CSF may reveal lymphocytic pleocytosis or oligoclonal bands. Acute ischaemic stroke involving the frontal lobe may demonstrate focal neurological deficits, with corresponding abnormalities on MRI. New-onset psychosis, absence of family history of psychiatric disease, and negative CSF and imaging should prompt the consideration of organic causes.
2-Deoxy-2-[18F] fluoro-D-glucose PET (FDG-PET) may serve as a useful adjunct to MRI, lumbar puncture, and EEG in the diagnostic evaluation of HSE, as well as for disease prognostication. It identifies and monitors inflammatory processes by measuring the brain glucose metabolism. Hypermetabolic regions may indicate active inflammation during the acute phase of encephalitis, while hypometabolic regions may reflect neuronal dysfunction caused by chronic inflammatory processes.11
A case-control study reported significant long-term recovery of frontal lobe-related cognitive deficits in patients with HSV encephalitis. However, subjective perceptions of cognitive recovery remained poor, with lethargy reported as a prominent complaint. This discrepancy between objective and patient-perceived cognitive improvement highlights the importance of post-encephalitis neuropsychological rehabilitation.12 Following appropriate treatment for HSE, the patient made a full recovery, suggesting that the neurological impairments associated with HSE may be reversible with early recognition and timely antiviral therapy.
CONCLUSION
This case illustrates an atypical presentation of HSV encephalitis with predominant frontal lobe dysfunction without classical temporal lobe involvement. The presence of neuropsychiatric symptoms and frontal lobe dysfunction may pose a diagnostic challenge, as it can mimic conditions such as autoimmune encephalitis, stroke, and primary psychiatric disorders. Early initiation of antiviral therapy in suspected cases while awaiting diagnostic tests is important, as it may reverse neurological dysfunction and improve clinical outcomes.
PATIENT PERSPECTIVE
“The abrupt onset of my symptoms came as a complete surprise to both my family and me. It was a distressing and disabling experience that significantly impacted my life. I am sincerely grateful for the comprehensive treatment and attentive care provided by the healthcare team throughout my hospitalisation. I hope that sharing my experience will enhance awareness of atypical frontal lobe presentations in HSE and ultimately contribute to improved patient outcomes.”






