Abstract
Heart failure with preserved ejection fraction (HFpEF) is a complex disease that has been historically difficult to treat and manage. Novel research shifts understanding of HFpEF from a primary heart disease to a systemic syndrome driven by systemic inflammation, congestion, and multi-organ metabolic dysregulation. These three key drivers can all be integrated into the heart–liver–pancreas inflammatory axis, with bidirectional self-amplifying interactions between these organs leading to a vicious cycle with worse clinical outcomes. This paper will unravel the mechanics of this axis and provide important implications from a therapeutic standpoint, shifting the management of HFpEF from cardiac-centric strategies to interventions targeting the underlying systemic inflammation, metabolic dysregulation, and congestion.
Key Points
1. Heart failure with preserved ejection fraction (HFpEF) has been the ‘greatest unmet need’ in cardiology due to its complex pathophysiology, the lack of targeted therapies in the disease, and the futility of cardiac-centric agents.2.This narrative explores the cardiac–hepatic–pancreatic axis proposed in HFpEF pathogenesis, and offers therapeutic implications illustrated by the benefits of novel therapies such as glucagon-like peptide-1 receptor agonists and sodium-glucose co-transporter 2 inhibitors.
3. Future HFpEF trials should assess metabolic and pancreatic markers to clarify whether this axis represents the true pathophysiology of HFpEF or is just an indirect association.
INTRODUCTION TO THE HEART–LIVER–PANCREAS AXIS
Heart failure with preserved ejection fraction (HFpEF) has historically been a troublesome condition to study and manage because of the variable presentation of the condition and the limited number of disease-modifying therapies to address it. HFpEF has conventionally been thought of as a problem of diastolic dysfunction and stiffness of the heart.1 However, the concept of HFpEF is progressively expanding to encompass a systemic disorder that is mediated by the principles of inflammation, congestion, and metabolism, and not simply a condition of the heart. The integrative theory of a connection between the heart, liver, and pancreas through the principles of a common axis of inflammation and haemodynamics is a significant contemporary contribution to the understanding of the pathophysiology
of HFpEF.
DISCUSSION AND OPINION ON THE HEART–LIVER–PANCREAS AXIS AND ITS INFLAMMATORY PATHWAY IN HFpEF
One of the major advantages of this model is the emphasis on venous congestion with low-grade systemic inflammation. Hepatic congestion in HFpEF is more than simply an association with right-sided heart failure; rather, it plays an active pathogenic role in disease progression.2 Elevation of sinusoidal pressures, hepatocellular hypoxia, and secondary fibrosis lead to congestion hepatopathy, which advances to cardiogenic cirrhosis in end-stage disease.2,3 The inflammatory derangement secondary to hepatic pathophysiology, with increased nitric oxide signalling, cytokine expression, and shifts in the hepatokine profile, generates a vicious cycle that reinforces the pathogenesis of myocardial disease and endothelial damage. Interestingly, this vicious cycle has been borne out in emerging concepts redefining cirrhotic cardiomyopathy not as a new disease, but rather as a clinical manifestation of HFpEF.1-3
Pancreatic exocrine insufficiency (PEI) is prevalent in chronic heart failure but not always evaluated.4 Splanchnic hypoperfusion, venous congestion, autonomic derangements, and inflammation can injure the exocrine functions of the pancreas.4 PEI may result in malabsorption, micronutrient deficiencies, sarcopenia, and cachexia, exacerbating heart failure.4 Additionally, there has been evidence showing that observed weight loss and malnutrition in HFpEF are more complex phenomena that are not solely attributed to heart disease or the ageing process; potential modifications in the gastrointestinal system are also advocated.5 Pancreatic and cardiac inflammatory links are established in acute pancreatitis, in which systemic inflammatory responses (cytokines: IL-1β, IL-6, TNF-α) lead to limited diastolic reserve, microvascular ischaemic disorders, arrhythmias, and myocardial depression. Patients with HFpEF with reduced diastolic function and microvascular inflammation are likely more vulnerable to these conditions’ haemodynamic changes.4-6 Observational data linking acute pancreatitis to an increase in in-hospital mortality among patients with pre-existing heart failure underscore the clinical relevance of this interaction.7-9
The addition of metabolic dysfunction-associated steatotic liver disease further strengthens the three-organ model. Metabolic dysfunction-associated steatotic liver disease acts as an amplifier of inflammation, oxidative stress, and fibrosis, independently increasing cardiovascular risk and susceptibility to developing HFpEF.10 The secretion of pro-inflammatory adipokines from visceral and epicardial adipose tissue contributes to ventricular stiffness and endothelial dysfunction, whereas hepatic insulin resistance further stresses the endocrine pancreas. From the perspective of the authors, it would appear that HFpEF represents the cardiovascular expression of the metabolic-inflammatory syndrome.10-12
From a therapeutic standpoint, this integrative axis offers several important implications. First, it reinforces the limitations of heart-centric management strategies in HFpEF. Interventions targeting congestion, inflammation, and metabolic dysregulation across organs may yield greater benefit than therapies focused solely on ventricular mechanics. The growing evidence supporting sodium–glucose cotransporter-2 inhibitors and glucagon-like peptide-1 receptor agonists in HFpEF aligns well with this paradigm, given their pleiotropic effects on inflammation, adiposity, and organ crosstalk.13,14
Second, recognition of PEI in heart failure raises the possibility that pancreatic enzyme replacement and nutritional optimisation could represent low-risk, high-yield adjuncts in selected patients as an area deserving prospective evaluation. Importantly, this model also invites a paradigm shift in clinical culture towards interdisciplinary care. Patients with HFpEF frequently traverse cardiology, hepatology, and gastrointestinal services without an integrated framework linking their symptoms and organ dysfunction.14,15 An interdisciplinary care approach incorporating biomarker profiling and monitoring, advanced imaging, and nutritional assessment may allow earlier identification of patients trapped in this inflammatory tri-organ loop and enable more personalised interventions.
CONCLUSION AND FUTURE DIRECTIONS
Conceptualising HFpEF through the cardio-hepato-pancreas inflammatory axis, also known as the heart–liver–pancreatic axis, provides a cohesive and biologically plausible explanation for the complexity of this syndrome. It reframes HFpEF as a systemic disorder driven by congestion, inflammation, and metabolic dysregulation, with reciprocal organ injury perpetuating disease progression. Taken together, while further mechanistic and interventional studies are required, this integrative perspective represents an important step towards more effective, holistic management of HFpEF that acknowledges the heart as part of an interconnected network rather than an isolated, failing pump.
While a direct, well-established link between pancreatitis and HFpEF is limited, the pancreas is relevant to HFpEF largely through shared metabolic pathways, particularly Type 2 diabetes and insulin resistance, which are highly prevalent in HFpEF and contribute to systemic inflammation, endothelial dysfunction, and impaired myocardial energetics underlying exercise intolerance (forward failure).16 Chronic metabolic stress involving pancreatic β-cell dysfunction and ectopic fat deposition can amplify circulating inflammatory mediators that affect both cardiac and hepatic tissues, supporting the broader cardio–hepato–metabolic interaction framework.15,16 Having said that, pancreatitis itself remains an indirect and more speculative component, with its relevance primarily hypothesised through inflammatory overlap rather than robust epidemiologic or mechanistic HFpEF-specific evidence. (Figure 1) depicts a proposed cardio–hepato–pancreatic inflammatory axis linking metabolic dysfunction across these organs.
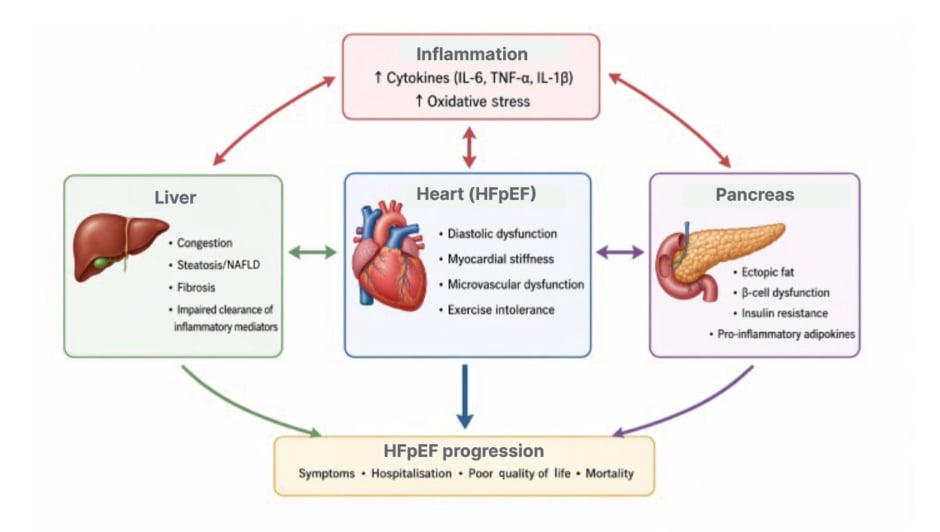
Figure 1: Reframing HFpEF through the cardio–hepato–pancreas inflammatory axis.
This figure shows HFpEF as a condition driven by a shared inflammatory network between the heart, liver, and pancreas. Inflammation and metabolic stress (like insulin resistance, fatty liver, and pancreatic dysfunction) interact to worsen heart stiffness, reduce exercise capacity, and promote congestion. Over time, these linked organ changes contribute to worsening symptoms, more hospitalisations, and poorer outcomes in HFpEF.
HFpEF: heart failure with preserved ejection fraction; NAFLD: non-alcoholic fatty liver disease.
While the hepatic and renal links are well supported by robust clinical and mechanistic evidence, the pancreatic component is largely inferential, based on shared pathways such as insulin resistance, systemic inflammation, and ectopic fat deposition rather than direct causal data.17 Given the current lack of strong epidemiologic or mechanistic evidence for pancreatic involvement, future HFpEF trials should include deeply phenotyped populations with metabolic and pancreatic biomarkers to clarify whether this axis reflects true pathophysiology or a secondary association.