BACKGROUND AND AIMS
While dual antiplatelet therapy (DAPT) effectively reduces thrombotic and ischaemic complications following percutaneous coronary intervention (PCI), it is associated with an increased risk of bleeding, particularly among patients with high bleeding risk (HBR).1 Although recent guidelines advocate abbreviated DAPT (≤3 months) in this population, the uptake of these strategies in routine clinical practice remains insufficiently described.2-4 The authors sought to assess real-world prescription patterns of abbreviated DAPT after PCI according to bleeding risk status, and to identify factors associated with prolonged DAPT use in patients with HBR using the nationwide FRANCE-PCI registry.5
MATERIALS AND METHODS
This analysis included consecutive patients undergoing PCI for acute or chronic coronary syndrome between 2014–2023 in 56 French centres participating in the prospective FRANCE-PCI registry.6 Patients alive at 1 year with available DAPT duration data were included. HBR was pragmatically defined by the presence of at least one of the following criteria: age ≥75 years, chronic oral anticoagulation, prior stroke, or chronic kidney disease. Multivariable mixed-effects logistic regression analysis was performed to identify predictors of prolonged DAPT (>3 months) among patients with HBR.
RESULTS
Among 115,992 patients included, 48,028 (41.4%) fulfilled HBR criteria. Despite guideline recommendations favouring shorter antiplatelet strategies in this population, abbreviated DAPT was prescribed in only 23.1% of patients with HBR compared with 3.6% of patients without HBR (p<0.001; (Figure 1).
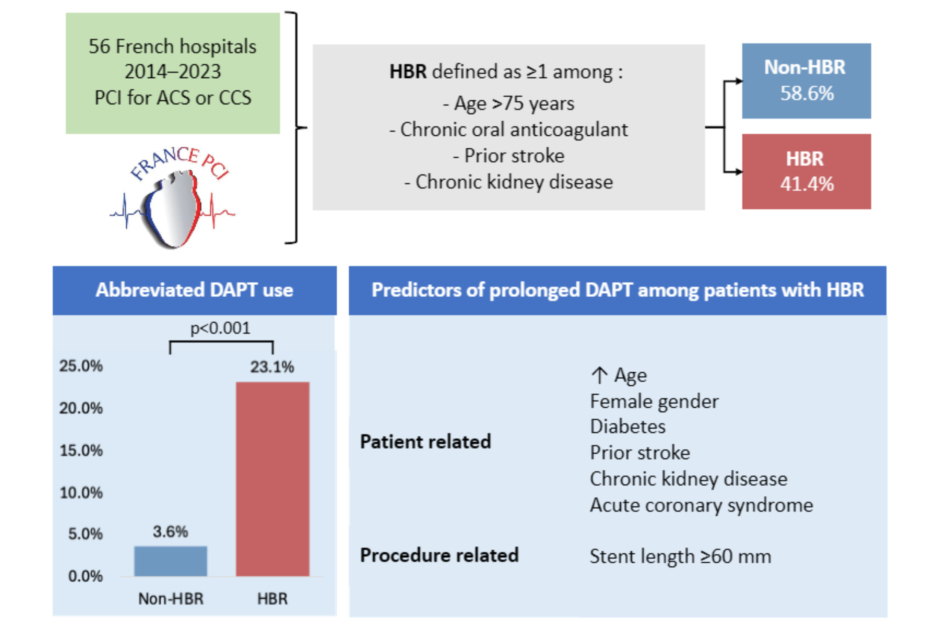
Figure 1: Real-world use of abbreviated DAPT after PCI in patients with HBR.
ACS: acute coronary syndrome; CCS: chronic coronary syndrome; DAPT: dual antiplatelet therapy; HBR: high bleeding risk; PCI: percutaneous coronary intervention.
Within the HBR subgroup, several clinical and procedural characteristics remained independently associated with prolonged DAPT use, including older age (odds ratio [OR]: 1.02; 95% CI: 1.02–1.03), female sex (OR: 1.18; 95% CI: 1.11–1.25), diabetes (OR: 1.15; 95% CI: 1.08–1.22), prior stroke (OR: 1.54; 95% CI: 1.39–1.69), chronic kidney disease (OR: 1.24; 95% CI: 1.15–1.34), acute coronary syndrome presentation (OR: 1.52; 95% CI: 1.44–1.61), and total stent length ≥60 mm (OR: 1.18; 95% CI: 1.09–1.28). Over the study period, abbreviated DAPT use progressively increased among patients with HBR, although prolonged DAPT remained the predominant strategy overall.
CONCLUSION
In this large, contemporary, nationwide PCI registry, fewer than one in four patients with HBR received abbreviated DAPT, despite current guideline recommendations. DAPT duration remained strongly influenced by markers of ischaemic and procedural complexity, underscoring the persistent challenges of balancing bleeding and ischaemic risks in routine clinical practice, and highlighting the gap between randomised trial evidence and real-world management.





