Abstract
Pulsed electromagnetic field (PEMF) therapy has emerged as a promising non-invasive modality for the management of osteoarthritis (OA), particularly as an adjunct to standard care. This narrative review examines current clinical evidence, mechanistic insights, and future directions for PEMF in OA based on a theoretical framework. Clinical studies consistently show encouraging results that PEMF reduces pain, stiffness, and functional limitations, supporting its role in symptomatic management. However, evidence for disease-modifying effects, such as cartilage preservation or regeneration, remains limited and inconclusive, with most trials underpowered relative to Phase III standards and characterised by substantial variability in treatment protocols.
Mechanistic studies indicate that PEMF modulates key biological pathways relevant to OA, including calcium–calmodulin-dependent nitric oxide signalling, inflammatory cytokine regulation, and metabolic reprogramming of chondrocytes. Emerging evidence further implicates targets such as hexokinase 2 and 15-hydroxyprostaglandin dehydrogenase in catabolic and regenerative processes. These findings suggest that PEMF has the potential to influence both symptom expression and underlying disease biology.
Building on these insights, the authors propose a framework for the rational design of targeted PEMF protocols based on molecular mechanisms and disease stage. Theoretical modelling of enzyme–substrate interactions provides preliminary estimates of field strengths required to modulate key enzymatic drivers of cartilage degradation. Such an approach, although computationally based and with inherent limitations, may facilitate the transition from empirically applied PEMF therapies to mechanism-based interventions. Future research should prioritise standardised protocols, mechanistic validation, and adequately powered clinical trials to fully evaluate the potential of PEMF as a disease-modifying therapy in osteoarthritis.
Key Points
1. Osteoarthritis is a leading cause of pain and disability, and current treatments primarily provide symptomatic relief without modifying disease progression.2. This narrative review summarises current clinical and mechanistic evidence on pulsed electromagnetic field (PEMF) therapy for osteoarthritis and proposes a mechanism-based framework for designing targeted PEMF protocols.
3. Current evidence supports PEMF as a safe adjunct for reducing pain and improving function, but disease-modifying effects remain unproven. A mechanism-informed approach to protocol design may improve future clinical outcomes and should be evaluated in adequately powered trials.
INTRODUCTION
In clinical practice, first-line pain management relies predominantly on pharmacological agents, including non-steroidal anti-inflammatory drugs (NSAID), corticosteroids, and opioids. These medications are effective for short-term relief but carry well-documented risks. Long-term NSAID use is associated with gastrointestinal injury, renal dysfunction, and increased cardiovascular risk.1 Corticosteroids can suppress immune function and promote osteoporosis, and opioids carry a substantial risk of dependency and addiction.2,3 Despite these limitations, pharmacological management remains the dominant approach for both acute and chronic pain.
These concerns have prompted growing interest in non-pharmacological alternatives. Physical therapy, acupuncture, mindfulness-based interventions, and dietary modification are increasingly recognised for their capacity to reduce pain and improve quality of life without systemic adverse effects.4 Among these alternatives, electromagnetic stimulation therapies have gained particular attention. Therapies such as transcutaneous electrical nerve stimulation and pulsed electromagnetic field (PEMF) therapy are becoming more widely used as drug-free pain relief solutions.5,6 The National Centre for Complementary and Integrative Health (NCCIH), part of the NIH, provides a public fact sheet discussing the use of magnetic fields for pain management, reflecting growing public and scientific interest in this field.7
This narrative review examines the emerging application of PEMF in osteoarthritis (OA), with particular attention to knee osteoarthritis. The authors summarise the available clinical evidence, mechanistic insights from preclinical studies, and current limitations of the field, before proposing a theoretical framework for future advances.
PEMF IN PAIN MANAGEMENT
What Is PEMF?
To understand PEMF therapy, it is helpful to distinguish it from static magnetic therapy (SMT). Although both approaches involve magnetic fields interacting with biological tissues, their mechanisms and clinical evidence differ substantially.
SMT uses permanent magnets that generate a constant, unchanging magnetic field. These magnets are typically embedded in bracelets, insoles, mattress pads, or wearable devices and placed on or near the body. The steady magnetic field may influence the alignment of charged particles in tissues and potentially affect ion transport across cell membranes. In SMT, the ‘dose’ is primarily defined by magnetic flux density, measured in Gauss (G) or Tesla (T). Most commercially available therapeutic magnets range from 300–5,000 Gauss. The depth of magnetic field penetration depends on both field strength and distance from the target tissue. However, despite widespread commercial availability, high-quality clinical evidence supporting SMT for pain relief remains limited. Published studies often report modest or inconclusive results, and SMT is considered less biologically active than time-varying electromagnetic therapies.
In contrast, PEMF therapy uses time-varying magnetic fields generated by electrical currents passing through coils. Because the magnetic field changes over time, it can induce small electrical currents within tissues (via electromagnetic induction). These induced currents are believed to stimulate cellular signalling pathways involved in inflammation control, tissue repair, and pain modulation. Compared to static magnets, PEMF devices can penetrate deeper into tissues, deliver dynamic electromagnetic stimulation, and allow precise control of multiple treatment parameters.
Key PEMF Control Parameters
Unlike SMT, PEMF dosing is defined by several independently adjustable variables: frequency, waveform, field intensity, and treatment duration.8 There are typically two frequency components in PEMF systems: the high-frequency electromagnetic oscillation within each pulse, often in the kHz or even MHz range, and the pulse repetition frequency (PRF), which is the rate at which pulses are delivered, typically ranging from a few Hz to several hundred Hz, depending on the application (e.g., bone healing versus pain management). Different frequencies may influence biological tissues in distinct ways.
The waveform or shape of the electromagnetic pulse, such as sinusoidal, square, rectangular, or sawtooth, may also alter the biological response. Waveform characteristics can affect how electrical currents are induced in tissues. The intensity or field strength is measured in Gauss or Tesla. Therapeutic PEMF devices can operate at low intensities (microtesla range) or significantly higher strengths, depending on the clinical indication. Finally, the duration of the treatment sessions typically lasts from minutes to over an hour, depending on the device and therapeutic goal. The total treatment course length may span daysto weeks.
Unlike static magnetic therapy, PEMF therapy is not defined by magnetic strength alone. Instead, its biological effects depend on the combination of frequency, waveform, intensity, and treatment duration. This multi-parameter control allows for more targeted therapeutic strategies, but it also makes comparing devices and clinical studies more challenging.
PEMF Dose-Response
As noted above, PEMF acts through magnetically induced tissue currents that alter ion movement and trigger downstream signalling. Decades of experimental research suggest that low-frequency pulsed fields are more bioactive than static magnetic fields, and that pulsed signals may produce stronger biological responses than continuous waveforms. Higher pulse repetition frequencies can enhance cellular responsiveness, while greater magnetic flux densities (within therapeutic ranges) tend to produce stronger biological effects. In addition, repeated exposure over multiple days, particularly beyond 10 days, amplifies cumulative responses. When waveform data are available, triangular waveforms have sometimes demonstrated stronger cellular effects compared to sinusoidal or square waves.
A meta-analysis of 92 studies demonstrated that PEMF responsiveness varies considerably by cell type and tissue origin.8 Interpretation of this literature is complicated by inconsistent reporting of key parameters, including waveform, pulse duration, frequency, and field strength, which limits cross-study comparisons and slows progress towards standardised protocols.6
CLINICAL TRIALS SUPPORTING EFFECTIVENESS IN OSTEOARTHRITIS, INCLUDING KNEE OSTEOARTHRITIS
Evidence supporting the use of PEMF for pain reduction and functional improvement in musculoskeletal conditions, including OA, is summarised in a health fact sheet produced by the National Centre for Complementary and Integrative Health (NCCIH).7 The cautious recommendation by the NCCIH that ‘Electromagnetic therapy may be a beneficial complementary therapy for treating osteoarthritis’ was based primarily on the meta-analysis of 12 clinical studies by Wu et al.9 and the systematic review of 15 additional studies by Paolucci et al.10 encompassing a total of 1,370 patients with osteoarthritis affecting primarily the knees, ankles, hands, neck, and lower back. Overall, these studies showed that electromagnetic therapy (mostly PEMF) reduced pain, improved physical function and reduced stiffness while being well tolerated. It could be a useful addition to the standard of care currently available to patients, although much remains to be done in optimising protocols and validating them with larger trials.
Since these reviews, several additional randomised controlled trials have been published, reflecting sustained interest in PEMF as a therapeutic modality.Table 1 summarises the key characteristics of these trials. Hashemi et al.11 conducted a small study with 70 female patients with primary knee OA. It investigated the effect of low-frequency PEMF in addition to a regular schedule of physical therapy. Exposure was 30 minutes every weekday for 3 weeks. Evaluations were conducted at baseline, after 3 weeks of treatment, and at 7 weeks of follow-up. The results showed that the PEMF group experienced less pain as measured by the Visual Analog Scale (VAS), lower functional limitation, and reduced stiffness at 7 weeks compared to the sham group. Sham refers to a fake therapeutic intervention that looks, feels, and sounds identical to the real treatment being tested, but deliberately omits the active component to serve as a baseline comparison. Physician Global Assessment (PGA) scores were also superior in the PEMF group versus sham. Similar to the previous study, Wang et al.12 investigated the effect of PEMF in a group of 60 patients with confirmed end-stage osteoarthritis (Kellgren–Lawrence [KL] Grade ≥3) in one or both knees. PEMF treatment was administered in addition to home-based stretching and strengthening exercises designed by physiotherapists. PEMF treatment consisted of two 10-minute sessions per week for 8 weeks, delivered by a Quantum Tx machine (QuantumTX, Singapore) generating a uniform 1 mT field intensity at 50 Hz pulse frequency. Both knees were treated in alternate sessions, so each knee was exposed to a total of 8 sessions. Evaluations were conducted at baseline and at 4 and 8 weeks of treatment. The results showed improved knee muscle strength and reduced pain, as well as a promising tendency to improve performance-based physical function (as measured by 6-metre walk plus sit-to-stand time) in the PEMF group versus sham.
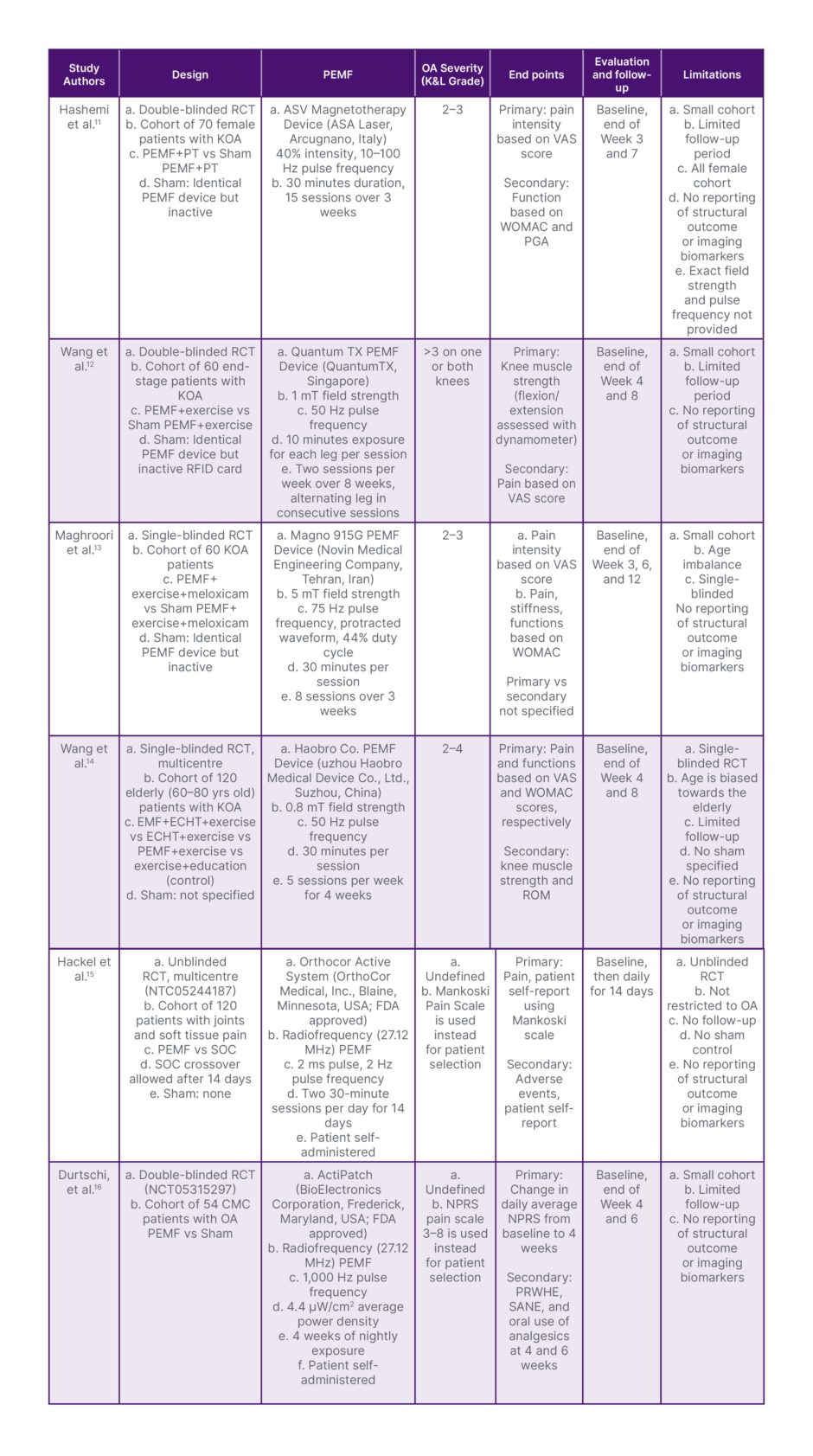
Table 1: Characteristics of recent PEMF therapy clinical trials (2024–2026) in osteoarthritis.
CMC: carpometacarpal; ECHT: external Chinese herbal therapy; KOA: knee osteoarthritis; NPRS: numeric pain rating scale; OA: osteoarthritis; PEMF: pulsed electromagnetic field therapy; PRWHE: Patient-Rated Wrist/Hand Evaluation; PT: physical therapy; RFID: radiofrequency identification; ROM: range of movement; SANE: Single Assessment Numeric Evaluation; SOC: standard of care; VAS: visual analog scale; vs: versus; WOMAC: The Western Ontario and McMaster Universities Osteoarthritis Index.
Collectively, these studies support supplementing standard physical therapy with PEMF in knee OA. Effective protocols used field intensities not exceeding 10 mT and frequencies below 100 Hz, with sessions of 10–30 minutes delivered two to five times weekly for up to 8 weeks. The durability of the benefit beyond this period and the need for maintenance sessions remain to be established.17
Maghroori et al.13 further investigated the utility of PEMF as adjunct therapy in a more complex setting where the patient population was already subjected to two forms of therapy: an exercise regimen plus a nonsteroidal anti-inflammatory drug, meloxicam 15 mg daily. PEMF treatment consisted of a 30-minute session with a pulse intensity of 50 Gauss (5 mT) and a frequency of 75 Hz. Each patient in a group of 60 diagnosed with Grade 2 or 3 knee OA was treated with eight sessions of PEMF or sham PEMF over 3 weeks. Evaluations at baseline, end of treatment, and follow-up at 6 weeks and 3 months after treatment showed that the addition of PEMF therapy enhanced pain relief and physical function with no reported side effects. The findings support the use of PEMF as adjunct therapy for patients with knee OA who are concomitantly treated with exercise and an NSAID agent.
In a similar complex setting comprising a population of 120 patients suffering from knee OA, KL Grade ≥2, Wang et al.14 investigated the effect of adding PEMF to two established therapies in China: exercise and external Chinese herbal therapy (Sanqi Shengyu External Application Cream). The PEMF protocol was distinct in using a much higher magnetic pulse intensity of 800 mT at a pulse frequency of 50 Hz for 30 minutes. Patients in the PEMF group were treated for a total of 20 sessions over 4 weeks. Evaluations were conducted at baseline, end of treatment, and at 4-week follow-up. The results of 4 treatment arms (exercise only as control, exercise + PEMF, exercise + external Chinese herbal therapy, and combination of exercise + PEMF + external Chinese herbal therapy) showed that the combined therapy group demonstrated superior outcomes, especially at the 4-week follow-up. The beneficial effect of external Chinese herbal therapy alone was durable, while that of PEMF diminished over time after intervention. The exercise-only control group also showed significant improvements, but less pronounced than the active intervention groups.
Direct comparison of these two trials is not possible given differences in PEMF protocols and control design; nonetheless, both support the use of PEMF as an adjunct to multimodal regimens combining exercise and anti-inflammatory therapy. Systematic optimisation of dosing parameters, including carrier frequency, pulse intensity, and treatment duration, across specific clinical endpoints, will be essential for advancing PEMF as a treatment option. To that effect, Yang et al.18 reported that at fixed magnetic field intensity (3.8 mT), higher PEMF pulse frequency (75>50>8 Hz) resulted in better recovery in a rat model ofknee osteoarthritis.
Two further trials warrant separate consideration because of the distinct characteristics of the devices employed. Unlike the protocols described above, which use field intensities in the millitesla range and pulse frequencies below 100 Hz, these trials employed devices operating at a 27.12 MHz radiofrequency carrier with field intensities in the microtesla range and pulse frequencies between 2–1,000 Hz. Such devices are more accurately classified as pulsed radiofrequency or shortwave therapy systems; they retain the capacity to penetrate soft tissue and disrupt chronic pain signalling, but whether they operate through the same cellular mechanisms as conventional PEMF remains to be established. Whether the two distinct sets of protocols operate similarly at the cellular or molecular level remains to be determined for particular biological applications.
Hackel et al.15 reported a prospective study with 120 patients suffering from diverse soft tissue or joint pain (ankle, back, knee, wrist, elbow, shoulder, foot, hip, or neck), although knee pain predominated (43%). Patients were randomised, but the study was not blinded and included two arms: PEMF and standard of care (SOC). Patients in the PEMF arm self-administered the treatment with a commercial device (Orthocor Active System, Orthocor Medical, Blaine, Minnesota, USA) operating at 27.12 MHz carrier radiofrequency, pulse frequency of 2 Hz, pulse duration of 2 ms, and classified by the FDA as a short-wave diathermy device. The treatment consisted of daily 2-hour sessions for 14 days as per the manufacturer’s instructions. After 14 days, patients in the SOC arm were allowed to cross over. The two key endpoints for the study were efficacy, measured by changes in pain score from baseline, and safety, measured by the number of adverse events. The overall results showed that use of the Orthocor device was safe and led to significant reductions in pain and medication use compared to the standard of care for joint and soft tissue pain.Durtschi et al.16 reported on a single-centre, double-blind RCT with 61 patients suffering from thumb carpometacarpal (CMC) osteoarthritis to test the effectiveness of another commercial PEMF device, the ActiPatch® made by BioElectronics Corporation, Frederick, Maryland, USA, classified by the FDA as a Non-Thermal Shortwave Device. The device operates at a 27.12-MHz carrier radiofrequency, a pulse frequency of 1,000 Hz, and a pulse duration of 0.1 ms. The study consisted of two arms: patients in a treatment group wore the device overnight for 4 weeks, whereas patients in the control group similarly wore a sham device that did not emit the radio waves. Two endpoints were considered: pain reduction and function improvement. Evaluations were conducted at baseline, at 4 weeks, at the end of treatment, and at 6 weeks of follow-up. The results showed that both PEMF and sham groups achieved pain reduction and function improvement at the end of treatment (4 weeks), but no statistical difference could be discerned between the two groups. At 6-week follow-up, however, the pain reduction was sustained in the PEMF group only. The placebo effect was substantial but did not extend beyond the treatment period.
Collectively, these studies suggest that PEMF therapy may provide moderate symptomatic benefits in osteoarthritis, particularly for pain reduction, improvement in physical function, enhancement of muscle performance in advanced disease, and reduction in analgesic utilisation. However, the evidence base remains constrained by methodological heterogeneity, relatively small cohorts, and short-term follow-up. Current clinical evidence is stronger for symptomatic management than for demonstrating true disease-modifying effects on osteoarthritis progression. Future trials would benefit from larger multicentre cohorts, standardised PEMF dosing protocols, robust sham controls, long-term imaging endpoints, biomarker-based assessments of cartilage preservation and inflammation, and stratification by OA phenotype and severity.
Mechanistic Aspects
Early mechanistic studies identified three principal effects of PEMF on inflamed joint tissues.19-21 First, PEMF modulates the calmodulin (CaM)-dependent nitric oxide (NO) signalling cascades in cells of inflamed joints, leading to an increase in the production of anti-inflammatory cytokines (e.g., IL-10, IL-13, sIL-1R) and a decrease in pro-inflammatory cytokines (e.g., IL-1 α/β, IL-6, TNF-α) by inhibiting the NF-κB pathway. The overall effect is a decrease in physiological pain mediators (bradykinin, prostaglandins, histamine) and enzymes responsible for degrading the cartilage matrix (matrix metalloproteinases [MMP] and ADAMTS). In addition, PEMF up-regulates the adenosine receptors A2A and A3 to stimulate chondrocyte proliferation, differentiation, and extracellular matrix synthesis through the release of anabolic morphogens, such as bone morphogenetic proteins and anti-inflammatory cytokines. Finally, acting through calmodulin (CaM)-dependent nitric oxide (NO) signalling cascades, PEMF also increases microvascular perfusion and oxygenation of tissues.
More recent work has further characterised the molecular responses of osteoarthritic tissue to PEMF. Using a cellular model of human chondrocytes (C28/I2) stimulated with IL-1β and a mouse model of osteoarthritis, Zhou et al.22 demonstrated that upregulation of SIRT1 (a transcription factor deacetylase) by PEMF blocks the activation of the pivotal pro-inflammatory NF-κB signalling pathway, which is often overactive in osteoarthritic joints. This finding is significant: it identifies a discrete molecular mechanism by which PEMF suppresses joint inflammation and potentially slows disease progression, and it reinforces NF-κB inhibition as a therapeutic target in OA.
Working with primary human chondrocytes, Bao et al.23 showed that the glycolysis rate increased in chondrocytes from arthritic cartilage, accompanied by upregulation of hexokinase II (HK2). Overexpression of HK2 promotes an inflammatory response and catabolism while inhibiting anabolic activities. Concomitant with the increased expression of HK2 was a decrease in expression of HMGA2, a DNA-binding protein capable of transcriptional regulation. The authors also showed that PEMF inhibits the expression of HK2 and increases HMGA2, leading to a reversal of the inflammatory and catabolic state in the chondrocytes. Lonidamine, an inhibitor of HK2, performed similarly. In a mouse model of osteoarthritis, lonidamine in combination with PEMF more effectively reversed cartilage degeneration. Finally, HK2 was proposed as a potential target for developing therapeutic agents for the treatment of osteoarthritis.
The beneficial effects of PEMF extend beyond bone and cartilage to tendons and periarticular muscle. Because tendinopathy and muscle atrophy increase mechanical stress on joints and contribute to OA progression, mechanistic findings in these tissues are directly relevant to the joint disease context.
Using proteomic analysis of rat muscles subjected to experimentally induced tendinopathy, Torretta et al.24 reported that glycolysis in these tissues is enhanced. When exposed to PEMF, changes in the pattern of cellular proteins support a switch towards oxidative phosphorylation, as evidenced by the increase in lactate dehydrogenase B (LDHB), which converts lactate to pyruvate, boosting NAD+ signalling, ATP production, and beta-oxidation of fatty acids. PEMF also increases the level of antioxidant proteins, which control the damage caused by reactive oxygen species. Two key transcriptional co-activators, PGC-1α and YAP, were upregulated by PEMF. The former is clearly linked to the increase in oxidative metabolism, anti-inflammatory state, and antioxidant effects. The latter supports tissue repair and regeneration, and cell proliferation.25
DISCUSSION
Clinical Trials and Mechanistic Insights
The expanding body of clinical evidence supports the use of PEMF therapy as an adjunctive intervention in osteoarthritis, particularly in combination with standard care, including physical therapy and pharmacological management. Across studies, PEMF has consistently demonstrated promising efficacy in reducing pain and inflammation, outcomes that are clinically meaningful and directly relevant to patient quality of life. However, evidence supporting structural modification of joint tissues, such as cartilage preservation or regeneration, remains limited and confined to preclinical models.
At present, clinical data supporting disease-modifying effects of PEMF remain insufficient and inconsistent. Most trials involve small cohorts, typically no more than several hundred patients, rendering them more comparable to Phase II studies than to adequately powered Phase III trials required for regulatory approval. Accordingly, no PEMF devices or treatment protocols have received full U.S. FDA approval as disease-modifying therapies for osteoarthritis. Consistent with this evidence base, PEMF is currently positioned from a regulatory standpoint as a non-invasive adjunct for symptomatic management. Several systems (e.g., ActiPatch, OrthoCor, and related wearable or wrap-based devices) have been FDA-cleared for the management of musculoskeletal pain, including knee OA; however, their indications remain restricted to symptom relief rather than modification of the underlying disease process.
A major limitation of the current clinical literature is the substantial heterogeneity in PEMF protocols, including differences in carrier and pulse frequencies, field intensities, waveforms, and treatment duration. This variability complicates cross-study comparisons and limits the interpretability of meta-analyses, thereby impeding the development of standardised treatment guidelines. Progress will require a more systematic classification of PEMF protocols grounded in biological mechanisms and aligned with defined clinical endpoints, distinguishing, for example, parameters optimised for symptom relief from those intended to modify disease progression.
Mechanistic studies provide a critical foundation for such an approach and have identified several biological pathways responsive to PEMF exposure. Broadly, these investigations cluster into two amplitude regimes. The first involves millisecond radiofrequency pulses (e.g., 27.12 MHz) with magnetic field strengths in the microtesla range. These protocols have been shown to promote calcium–calmodulin (Ca²⁺/CaM) interactions and activate nitric oxide (NO) signalling cascades, resulting in downstream anti-inflammatory and anti-catabolic effects in diseased joint tissues.
A second body of work has examined PEMF protocols characterised by magnetic field strengths in the millitesla range and pulse frequencies below 100 Hz. Applied across a range of biological systems, including chondrocytes, stem cells, articular cartilage, tendons, and ligaments, these protocols consistently demonstrate anti-inflammatory and anti-catabolic effects as well as regenerative responses. These include enhanced extracellular matrix synthesis and an increase in cartilage and subchondral bone thickness.10,19 Taken together, these findings suggest that PEMF has the capacity in preclinical disease models to engage both symptom-modifying and tissue-restorative processes, a combination that is highly relevant to osteoarthritis pathophysiology.
Potential modes of action include modulation of intracellular signalling cascades, transcriptional regulation, and direct perturbation of molecular interactions; however, these mechanisms have not yet been integrated into a unified framework. Continued reliance on heterogeneous and empirically derived protocols risks generating fragmented insights, thereby limiting mechanistic clarity and slowing clinical translation.
Addressing these limitations will require a strategic shift in both clinical and pre-clinical research. Future clinical trials should be scaled for larger patient populations, comparable to Phase III studies, and incorporate more rigorous stratification by disease stage. Critically, these patient subgroups should be prospectively matched with PEMF protocols designed to target specific biological processes. In parallel, mechanistic studies should transition toward hypothesis-driven designs in which stimulation parameters are selected based on established features of osteoarthritis pathology.
Such an integrated, mechanism-informed framework would enable a more precise definition of therapeutic parameters, improve reproducibility across studies, and enhance clinical efficacy. This approach could reposition PEMF from an empirically applied adjunct therapy to a rationally designed, mechanism-based intervention with the potential to achieve disease modification in osteoarthritis.
Targeted PEMF TherapyFor Osteoarthritis
OA is driven by a combination of biomechanical stress and cellular senescence, leading to metabolic reprogramming within joint tissues. This altered cellular state promotes a phenotype characterised by chronic inflammation and progressive degradation of articular cartilage, resulting in pain, functional impairment, and reduced mobility. Inflammatory signalling is mediated in part by pro-inflammatory cytokines, primarily IL-1β, TNF-α, and IL-6, which stimulate the production of pain mediators (e.g., bradykinin, prostaglandins, histamine) as well as matrix-degrading enzymes, including ADAMTS family members and MMPs. Pharmacological strategies targeting downstream mediators, particularly prostaglandins, have achieved clinical success and form the basis of current symptomatic treatments. In contrast, efforts to directly target upstream cytokines have failed, reflecting both the multifactorial nature of OA and redundancy within inflammatory signalling networks. In addition, inadequate patient stratification in clinical trials may have obscured potential benefits, as patients with a strong inflammatory endotype were diluted within more heterogeneous study populations.26,27
These limitations have prompted a shift toward targeting structural drivers of disease progression, particularly cartilage-degrading enzymes. OA progression is increasingly understood as a sequential process involving initial inflammation and cytokine activation, followed by aggrecan degradation, mechanical weakening of cartilage, and collagen breakdown. This framework suggests a stage-specific therapeutic strategy, in which aggrecanase inhibitors (notably ADAMTS-5 and, to a lesser extent, ADAMTS-4) may be most effective in early disease, whereas collagenase inhibitors (e.g., MMP-13, with contributions from MMP-3 and MMP-1) may be required to limit structural deterioration in more advanced stages.28,29-31 Additional enzymes, such as ADAMTS-7, may contribute to matrix degradation through effects on cartilage oligomeric matrix protein (COMP), although their therapeutic relevance remains less clearly defined.32
Beyond matrix degradation, metabolic dysregulation has emerged as a key feature of OA pathophysiology. Notably, upregulation of 15-hydroxyprostaglandin dehydrogenase (15-PGDH), the principal enzyme responsible for prostaglandin E₂ (PGE₂) inactivation, may limit endogenous repair processes despite the known regenerative roles of PGE₂ in stem cell function, tissue repair, and cell survival. Inhibition of 15-PGDH by SW033291 resulted in cartilage regeneration in experimental models of OA.33 Additional translational studies could lead to the development of drugs addressing cartilage repair and regeneration in patients with OA. Concurrently, increased glycolytic activity in osteoarthritic chondrocytes, driven in part by HK2, has been linked to a pro-inflammatory, catabolic phenotype.23 Importantly, recent experimental evidence suggests that inhibition of HK2, particularly in combination with PEMF, can attenuate cartilage degeneration in preclinical models. Together, 15-PGDH and HK2 represent promising targets for restoring metabolic balance and promoting tissue regeneration in OA.23,33
Against this backdrop, the development of PEMF protocols designed to modulate specific enzymes represents a mechanistically grounded therapeutic strategy. A rational development pathway would involve initial characterisation of PEMF effects on enzyme kinetics in vitro, followed by validation in relevant animal models, and translation into human clinical studies. Conceptually, electromagnetic fields may influence enzyme function by perturbing enzyme–substrate interactions. This can be framed in energetic terms: disruption may occur when the energy imparted by the electromagnetic field approaches or exceeds the standard free energy of binding (ΔG⁰), which can be estimated from equilibrium constants (Keq). In most enzymatic reactions, Keq could be approximated using the Michaelis–Menten Km values since the kcat component tends to be negligibly small. By relating ΔG⁰ at the molecular level to the potential energy experienced by dipole moments within enzyme–substrate complexes (μE: ΔG0/N), it becomes possible to estimate the electric and magnetic field strengths required for functional disruption.34
The calculations summarised in Table 2 provide preliminary estimates of the static magnetic field intensities required to disrupt interactions between key enzymes and their substrates in OA. Although these values are based on simplifying assumptions and should be interpreted cautiously, they offer a quantitative framework for linking PEMF parameters to specific molecular targets. Notably, the estimated field strengths suggest that early-stage disease (KL Grade 1, doubtful joint space narrowing and possible osteophyte lipping) may be amenable to protocols delivering local magnetic fields in the 10–30 mT range, sufficient to target aggrecanases (ADAMTS-5 and ADAMTS-4) and to modulate HK2-driven glycolysis. Such a dual-target approach could simultaneously reduce matrix degradation and rebalance chondrocyte metabolism, thereby slowing disease progression.
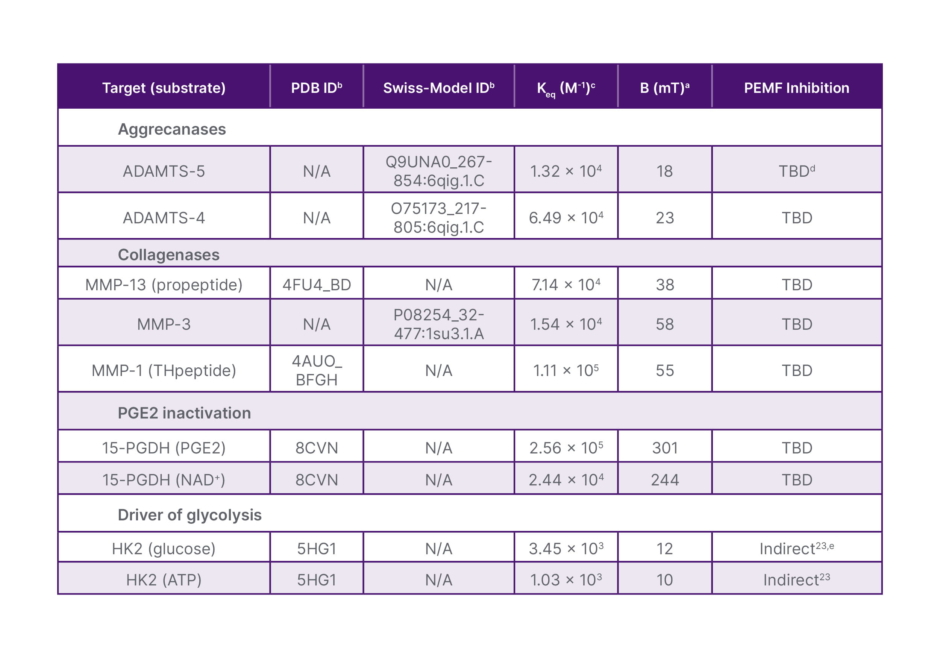
Table 2: Estimated static magnetic field strengths required for disrupting interactions between enzymes and substrates responsible for cartilage degeneration.
aCalculation of B (mT) was performed as previously reported.34
bThe dipole moment (μ) of the proteins was calculated from coordinates provided in the corresponding PDB or Swiss-Model files shown. Charge distribution at pH 7.4 of the appropriate protein chain(s) and bound ligands was first calculated using the PDB2PQR module of the APBS server.35 The resulting .pqr file was subsequently read by a Python script (dipole_calculator, available upon request), which computes the dipole vector following equation: 
cThe Keq used for calculating ΔG0 is 1/Km for enzyme-substrate interaction. The catalytic Km values used as a first approximation of substrate affinities were obtained from the following sources: ADAMTS-5,36,37 ADAMTS-4,36,38-40 MMP-13,38, 41-46 MMP-3,43 MMP-1,39,42-44, 46 15-PGDH,47-52 and HK2.53,54 A median was selected when multiple Km values were reported for variant synthetic substrates.
dProof of inhibition by PEMF to be determined empirically.
eIndirect proof of inhibition.33
APBS: Adaptive Poisson–Boltzmann Solver; ATP: adenosine triphosphate; B: static magnetic field strength (magnetic flux density); CoM: center of mass; ΔG°: Standard Gibbs free energy change; HK2: hexokinase 2; K_eq: equilibrium constant; K_m: Michaelis constant; mT: millitesla; MMP: matrix metalloproteinase; M⁻¹: inverse molar (per mole per liter); μ: electric dipole moment; N/A: not applicable; NAD⁺: nicotinamide adenine dinucleotide (oxidized form); PDB: Protein Data Bank; PDB2PQR: Protein Data Bank to Protein Quantity Relationship; PEMF: pulsed electromagnetic field; pH: potential of hydrogen; PGE₂: prostaglandin E₂; PQR: protein structure file format containing atomic coordinates, charges, and radii; TBD: to be determined; 15-PGDH: 15-hydroxyprostaglandin dehydrogenase.
As the disease advances (KL Grade 2, definite osteophytes and possible joint space narrowing), higher field strengths may be required to address collagen degradation. Table 2 indicates that inhibition of collagenases such as MMP-13, MMP-3, and MMP-1 may require magnetic fields in the 50–60 mT range, consistent with the smaller dipole moments of these enzyme–substrate complexes. In later stages, restoration of regenerative signalling through preservation of PGE₂ may necessitate even higher field strengths (300 mT) to inhibit 15-PGDH activity. Importantly, these estimated field strengths fall within the operational capabilities of existing PEMF technologies, including devices already approved or marketed for clinical and wellness applications. However, it is equally important to emphasise that therapeutic efficacy is unlikely to depend on field strength alone; rather, optimal outcomes will require careful integration of multiple parameters, including frequency, pulse structure, duty cycle, and treatment duration.
Taken together, the framework summarised in Figure 1 supports a conceptual shift from empirically applied PEMF protocols towards rationally designed, target-specific interventions. By aligning PEMF parameters with defined molecular mechanisms and disease stages, it may be possible to enhance therapeutic precision, improve clinical outcomes, and position PEMF as a viable strategy for disease modificationin osteoarthritis.
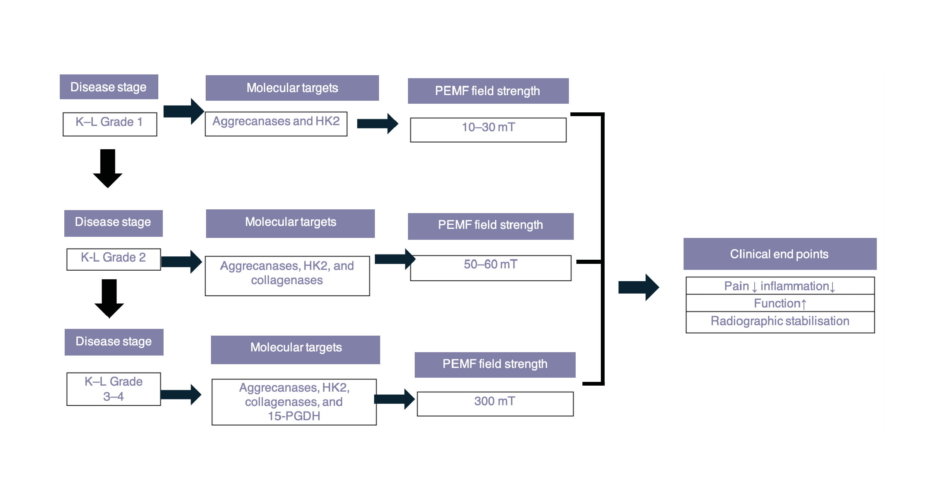
Figure 1: Rational framework for PEMF treatment at various OA stages.
15-PGDH: 15-hydroxyprostaglandin dehydrogenase; HK2: hexokinase-2; K–L: Kellgren–Lawrence; mT: millitesla;
OA: osteoarthritis; PEMF: pulsed electromagnetic field.
CONCLUSION
PEMF therapy represents a non-invasive and well-tolerated adjunctive therapy for OA, with current clinical evidence supporting symptomatic benefit, principally pain reduction and functional improvement, when used alongside physical therapy and pharmacological management. It should be noted, however, that disease-modifying effects, including structural preservation of articular cartilage, remain unproven. No trial to date has demonstrated that PEMF alters the natural history of osteoarthritis, and this distinction between symptomatic and disease-modifying activity must be maintained in interpreting theavailable evidence.
A central challenge in the field is the persistent lack of protocol standardisation, which continues to limit reproducibility and cross-study comparability. Addressing this will be a prerequisite for any credible progression towards disease-modifying claims. Alongside this, advances in the mechanistic understanding of PEMF, particularly its effects on inflammatory signalling, matrix degradation, and metabolic dysregulation, provide a rational basis for the development of more precisely targeted protocols.
The framework proposed in this review is best understood as hypothesis-generating. By integrating biophysical modelling with mechanistic insight, it identifies specific molecular targets, including aggrecanases, collagenases, and metabolic regulators such as HK2 and 15-PGDH, that may, in principle, be amenable to PEMF-based modulation. These proposals have not been validated experimentally, and the field strength estimates derived from enzyme–substrate modelling carry inherent limitations. The value of this framework lies not in its predictive precision, but in its capacity to generate testable hypotheses and to reorient PEMF research from empirical application towards mechanism-informed design.
Ultimately, realising the full potential of PEMF in osteoarthritis will require coordinated progress in protocol standardisation, patient stratification, and adequately powered clinical trials. For now, PEMF should be regarded as a promising and well-tolerated adjunct for symptom management, and the mechanistic framework advanced here as a starting point for hypothesis-driven investigation. Whether PEMF can achieve disease modification in osteoarthritis remains an open question, one that the field is not yet equipped to answer, but which a more rigorous, mechanism-informed research agenda may, in time, resolve.






