BACKGROUND AND AIMS
Survivors of severe COVID-19 may exhibit immune dysregulation, characterised by reduced naïve and increased senescent and exhausted T cell populations.1 Regular exercise is associated with increased naïve and reduced exhausted and senescentT cell populations, and may thereforehelp resolve post-COVID-19immune dysregulation.
The aim of this study was to explore the effect of an 8-week exercise-based rehabilitation intervention on cluster of differentiation (CD)4 and CD8 T cells and subsets in participants with post-COVID syndrome following hospitalisation, compared with usual care.2
MATERIALS AND METHODS
This was a sub-study in a single-blind RCT comparing an 8-week supervised rehabilitation programme to usual care alone. The rehabilitation programme consisted of twice weekly, individually prescribed and progressed aerobic and strength training, and a programme of education/self-management techniques, supplemented by a home exercise programme. Venous blood samples were collected pre- and post- intervention, and T cell immunophenotyping via flow cytometry was performed and analysed using linear mixed models.
RESULTS
Thirty-one participants (n=13 male; 42%) completed blood samples pre- and post- intervention: 13 in the rehabilitation group and 18 in usual care alone. At 8 weeks, there were statistically significant differences in the number of central memory and naive CD8+ T cells, with an increase observed in rehabilitation and a decrease observed in usual care (all p<0.05; Figure 1). The number of CD8+ effector memory T cells increased in rehabilitation only (p<0.05), with no change in usual care alone (Figure 1). There were statistically significant differences in natural killer cells in the rehabilitation group compared to usual care alone (mean [CI]; rehabilitation pre: 271 [198–345] cells/µL; rehabilitation post: 378 [298–459] cells/µL; usual care pre: 302 [236–367] cells/µL; usual care post: 265 [200–331] cells/µL; p<0.05). There were no statistically significant differences in inflammatory and cardiometabolic biomarkers, including C-reactive protein, IL-6, cholesterol, triglycerides, and glucose.
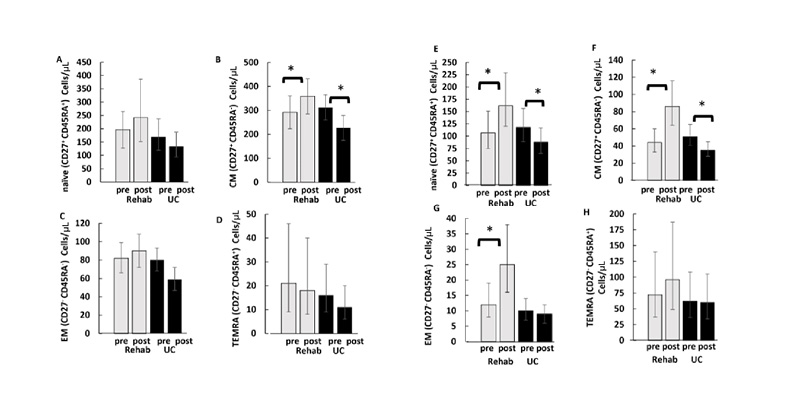
Figure 1: Effect of exercise versus usual care on cluster of differentiation 4+ (A–D) and cluster of differentiation 8+ (E–H) subset changes from pre- to post-trial.
*Significant difference from pre and within trial.
Data are mean (95% CI) and are adjusted for sex and baseline value of the dependent variable.
CD: cluster of differentiation; CM: central memory; EM: effector memory; TEMRA: terminally differentiated effector memory; UC: usual care.
CONCLUSION
Exercise-based rehabilitation could be a potential therapy for restoring post-COVID-19 immune dysregulation.






