Abstract
Rhinorrhoea is the excessive production of mucus commonly triggered by inflammatory or irritative conditions like bacterial infections and allergic rhinitis (AR). Factors such as hormonal changes and structural issues, including cerebrospinal fluid leakage, are also contributors. This report presents a case of seasonal AR successfully treated with allergen-specific immunotherapy for grasses and rye. During the past 5 years, the patient experienced intermittent perennial AR symptoms through a moderate sensitisation to house dust mites, managed by medication. Recently, progressive bilateral rhinorrhoea occurred, along with headache and muscle malaise. The complementary cranial MRI identified a pituitary macroadenoma with involvement of the optic chiasm. Surgical removal of the adenoma and nasopharynx reconstruction resolved the symptoms, confirming the cerebrospinal fluid rhinorrhoea. This case highlights that pituitary macroadenoma can masquerade as perennial AR, particularly when classic signs such as unilateral rhinorrhoea and visual disturbances, including diplopia and lateral vision loss, are absent. A cranial MRI can thus help prevent diagnostic delays and facilitate an appropriate treatment.
Key Points
1. Pituitary macroadenoma can be suspected in the absence of specific symptoms (unilateral rhinorrhoea, visual disturbances), although house dust mite sensitisation and bilateral rhinorrhoea can hide it.2. An appropriate radiological examination for chronic headache or persistent rhinorrhoea can avoid diagnostic delay, enabling an appropriate treatment.
3.The pituitary macroadenoma-related visual disturbances and unilateral cerebrospinal fluid rhinorrhoea can be absent even when the MRI reveals the corresponding structural alterations.
INTRODUCTION
Allergic rhinitis (AR) is an IgE-mediated immune response to inhaled allergens, like pollen, house dust mites (HDM), or pet dander, causing inflammation of the nasal airways.1-4 Symptoms include sneezing, nasal congestion, and an itchy, watery, runny nose (rhinorrhoea).1-3 Besides trigger avoidance, its management cornerstones include antihistamines and nasal steroid sprays, often lasting for seasons or year-round. Meanwhile, allergen-specific immunotherapy (AIT) is an aetiological treatment that suppresses symptoms, need for medication, and disease progression through immune modulation.1-3
Pituitary macroadenoma (PMA) is a benign tumour of the pituitary gland that causes clinical signs through the mass effect and increased intracranial pressure, including headache and hormonal imbalances.5-8 It induces additional diplopia and lateral vision loss by compressing the optic chiasm. When symptoms occur, the primary treatment is the surgical removal.5-9
Common causes of rhinorrhoea include inflammatory or irritative pathologies and hormonal changes, while structural alterations can be associated with cerebrospinal fluid (CSF) leakage.1-3,5,7-11 The aetiology determines the treatment, which includes the aforementioned antiallergics, as well as antibiotics, anti-leukotrienes, alpha-blockers, etc.1,2 We present a case of seasonal AR successfully treated with AIT that later experienced progressive chronic rhinorrhoea, resolved after PMA removal.
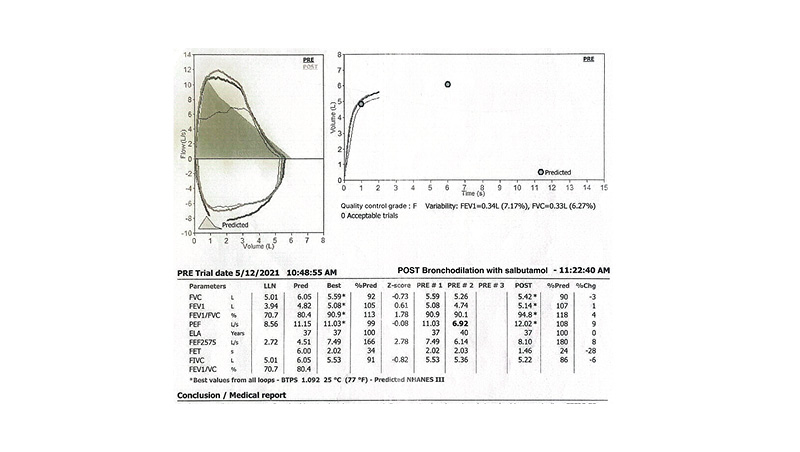
Figure 1: Spirometry results.
This examination revealed normal expiratory volumes and an obstructive pattern in the small airways, with insignificant response to salbutamol.
Best refers to maximal result.
BTPS: body temperature, pressure, saturated; Chg: change; FEF25-75%: forced expiratory flow between 25% and 75% of vital capacity; FEV1: forced expiratory volume within the first second; FIVC: forced inspiratory vital capacity; FVC: forced vital capacity; PEF: peak expiratory flow; Post: the maximal result after salbutamol spray; PRE: pre-bronchodilator; Pred: predicted; VC: vital capacity.
CASE PRESENTATION
A male patient born in the early 80s visited the clinic for specialised examination and treatment about 5 years ago. The patient had had seasonal AR since the age of 25 years, with sneezing, rhinorrhoea, itchy throat, and nasal congestion. Symptoms were present from late February–June, peaking in April and May, outdoors. Recently, before the first visit, the subject also experienced intermittent, nonseasonal, and moderate cough, sneezing, and rhinorrhoea, indoors. The treatment included oral antihistamines, intranasal decongestants, and intranasal glucocorticoids. The personal history noted arterial hypertension, and the family history was negative for atopic pathologies. The respiratory functional examination revealed normal expiratory volumes and an obstructive pattern in the small airways, with a nonsignificant response to salbutamol (Figure 1). Skin prick test resulted highly positive for grasses’ pollens, including cultivated rye, as well as moderately positive for HDM, hazel, and wall pellitory pollen (Table 1). Following these findings, the treatment comprised topical glucocorticoids and antihistamines. The IgE test (inhalation 30-l quantitative multiparameter assay [Polycheck® (bioCheck Gesellschaft für biologisch-immunologische Nachweisverfahren mbH, Münster, Germany)] for locally relevant Mediterranean allergens confirmed B2 grasses (Allergy Therapeutics, Worthing, UK), including cultivated rye, appropriate for AIT, which lasted for 3 years. The successful treatment brought the seasonal symptoms under control, except during the season’s peak, when the patient needed regular topical antihistamine and glucocorticoid medication (while outside the season, this was occasional).
Later, post-seasonally, a few months after AIT discontinuation, the patient experienced chronic moderate congestion and progressive but controllable watery rhinorrhoea, while other symptoms did not change. Justifiably, the nasal complaints corresponded to a moderate HDM sensitisation, as the nonseasonal symptoms predominated indoors. Within some weeks, together with (equally bilateral, turned refractory and tasteless) rhinorrhoea progression, the subject also complained of chronic headache, additional need for antihypertensives, muscular malaise, and general discomfort. The recommended cranial MRI by respective specialists identified a PMA with a circumferential diameter of 14 mm (anteroposterior) and 21 mm (transversal), mild compression of the optic chiasm and right optic nerve, with infiltration of the middle area of the right cavernous sinus, and a normal left one. Hormonal testing has detected prominent hyperprolactinemia, increased adrenocorticotropic hormone (ACTH) and cortisol levels, and slightly decreased testosterone and calcium levels (Table 2). Still, the haematoxylin and eosin examination supported the presence of a plurihormonal prolactin and ACTH neuroendocrine tumour, exhibiting a mixture of monomorphic, mostly chromophobic, and sparse granulated cells, generally in trabecular and sinusoidal structures. The administration of dopamine-synergist cabergoline protected the subject from the PMA-related hyperprolactinemia until the upcoming transsphenoidal surgery that followed a few weeks later. After a couple of months, a subsequent MRI revealed successful intervention, showing grafting in the sphenoidal sinus, malacia, and postoperative changes on the right side of the adenohypophysis without residual lesion. The sellar fossa showed enlargement, and the left side of the pituitary was homogeneous. Also, other related structures, including the infundibulum, suprasellar cistern, optic chiasm, and bilateral cavernous sinuses, were normal. Three months after the intervention, the patient still denied the persistent rhinorrhoea and is under periodical monitoring.
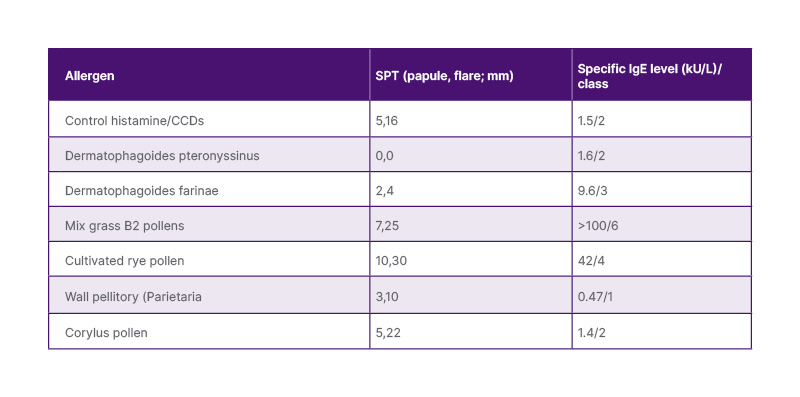
Table 1: The most relevant SPT (Allergy Therapeutics, Worthing, UK/Lofarma, Milan, Italy) and specific IgE (inhalation 30-l quantitative multiparameter assay [Polycheck® (bioCheck Gesellschaft für biologisch-immunologische Nachweisverfahren mbH, Münster, Germany)]) results.
CCD: cross-reactive carbohydrate determinant; SPT: skin prick tests.
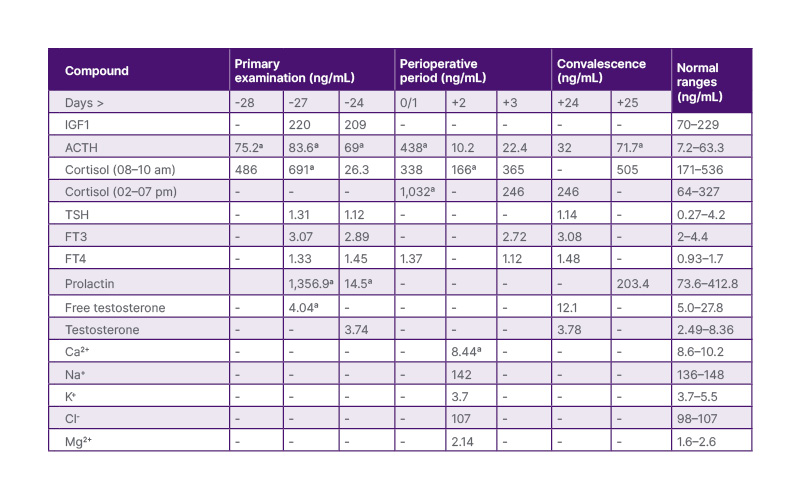
Table 2: Hormonal and electrolyte levels from PMA diagnosis to a few weeks after intervention.
ᵃAbnormal values (or alterations from normal ranges).
Cabergoline decreased prolactin levels before intervention.
ACTH: adrenocorticotropic hormone; Ca: calcium; Cl: chloride; FT: free triiodothyronine; IGF1: insulin-like growth factor 1; K: potassium; Mg: magnesium; Na: sodium; PMA: pituitary macroadenoma; TSH: thyrotropin-stimulating hormone.
DIFFERENTIAL DIAGNOSIS
Common causes of rhinorrhoea, including inflammatory pathologies (AR, bacterial rhinitis), irritant factors (cold air, tobacco smoke, medications), and rare cases (hormonal imbalances, structural deviations resulting from cranial trauma or increased CSF pressure) have been progressively explored.5-7 Together with diagnostic results, nonseasonal intermittent sneezing, nasal congestion, and watery rhinorrhoea can correspond with moderate perennial AR. In fact, watery rhinorrhoea characterises allergic and non-inflammatory pathologies, while the presence of sneezing, congestion, cough, and (almost seasonal) itchy throat supports the AR diagnosis.5-7,12 The recent non-allergological disease history excluded almost all the mentioned causes (tobacco smoke, medication abuse, cranial trauma, odours). Among nasal symptoms, only rhinorrhoea progressed over the recent month until surgical intervention. This showed positional variation, with gravitational aggravation at the lower side. There were no unusual taste alterations, even during the preoperative period. Unfortunately, the cholinergic or nasal allergic provocation tests were not in disposition. Probably, the moderate malaise was first considered an adverse effect of antiallergic medications. Finally, the rhinorrhoea turned refractory to the medications, and the progressive muscular malaise and headache required supplementary diagnostic procedures. The MRI determined the correct diagnosis, which further guided the authors to an appropriate treatment.7-11,13,14 In accordance with the hormonal findings, the histological examination confirmed a plurihormonal (prolactin and adrenocorticotropic hormone) adenoma sensitive to cabergoline.13,14
DISCUSSION
PMA is the most common suprasellar lesion in adults.5-7 This case shows that such adenomas and perennial AR are generally distinct conditions, but they can intersect in ways that complicate diagnosis and management.5-8 The most significant, though rare, intersection is when PMA-related CSF rhinorrhoea mimics a chronic AR.5,8-10 The authors’ case lacked specific unilateral persistent (and salty-tasting) nasal leakage during all allergist visits. So, the patient took medication for perennial AR, and afterwards followed the removal of PMA.5,6 The AR also implicates the neuronal structures, as immuno-allergic and neurogenic inflammation (mediated by the ophthalmic and maxillary branches of the trigeminal nerve), among others, induce bilateral watery rhinorrhoea, as in the authors’ case.1,3,15 Also, the domination of seasonal symptoms by AIT confirmed the AR over the years.
In contrast to AR, the PMA increases intracranial pressure, destroying the bony sella and dura, allowing CSF to escape through the altered nasopharyngeal side.6-10 The sellar compression and infiltration of the optic chiasm/nerve(s) can lead to diplopia or a narrowed visual field. The authors’ patient did not complain of such symptoms despite alterations detected on MRI, which predominated on the right, possibly because the compression and infiltration were clinically insignificant. The PMA removal was associated with sphenoidal sinus grafting to repair skull base defects and prevent CSF leakage.5-11 This successful intervention interrupted the persistent rhinorrhoea and any need for treatment. Muscular malaise is a nonspecific symptom, but in the authors’ case, it finally suggested a hormonal imbalance.5,6,8 Also, the headache, a non-specific symptom, has later been regarded as PMA-related because the patient had already been diagnosed and treated for arterial hypertension.8
CONCLUSION
This work emphasises that objective evidence of sensitisation does not exclude the atypical concurrent structural causes of rhinorrhoea, reinforcing the need for heightened clinical suspicion in patients with refractory, progressive, or treatment-discordant symptoms, even when an allergic diagnosis appears established. So, persistent rhinorrhoea, apart from being treated as allergic or chronic rhinitis, especially when other symptoms persist or develop, such as a watery (even non-unilateral) rhinorrhoea refractory to medication, warrants careful evaluation, as it can suggest other comorbidities, such as CSF leakage.






