Abstract
Background: The use of virtual reality and video games has gained traction in physical rehabilitation medicine. In respiratory rehabilitation, their use is more recent, and for the application of this tool in this area it is necessary to examine the intensity of the effort reached in the activity. To evaluate the intensity of effort achieved in the ‘Reflex Ridge’ Xbox 360™ (Microsoft, Redmond, Washington, USA) game compared to the current gold standard treatment, the cardiopulmonary exercise test (CPET), in asthmatic children.
Methods: A cross-sectional study evaluating children participating in a CPET and the Reflex Ridge active video game (AVG), played using an Xbox 360 Kinect,TM over two different days.
Results: Thirty children who had a mean age of 7.86±1.9 years were evaluated. The maximum heart rate using the AVG reached 87% of the maximum predicted value and 93% of that obtained in the CPET. The intensity of the exercise using AVG reached 8.46±1.86 MET; this corresponded to 81% of the intensity reached in the CPET. There were no episodes of exercise-induced bronchospasm.
Conclusion: Using AVG can promote high intensity physical exercise. AVG playing may be considered a safe mechanism for the physical treatment of asthmatic children.
INTRODUCTION
Physical exercise is an important non-pharmacological component of clinical asthma control, especially in children.1 However, physical exercise can lead to induced bronchospasm, which affects 40–90% of asthmatic children.1 In addition, physical exercise may not be motivating, and therefore these aspects may lead these children to adopt a sedentary lifestyle, which can worsen their clinical condition.2 Alternative forms of exercise, such as playful physical activities (e.g., interactive video games), can be beneficial as long as the patients are properly monitored and the activities are safe.
It is understood that playful physical activity provides physiological benefits for children with asthma provided that the activity fulfils three conditions: involves large muscle groups; is of moderate intensity, reaching at least 3–6 MET; and has a minimum duration of 20 minutes.3 This activity should also be applicable in clinical practice.4 It is important to emphasise that a playful and motivational physical activity may include active video games (AVG). Although the number of published studies involving asthmatic children is small, there are publications that show the potential of AVG in asthma treatment protocols.5-7
AVG has been highlighted as a form of physical activity with adequate intensity in the literature since Del Corral et al.8 compared the 6-minute walk test (6MWT) to three AVG and found that two of the three AVG imposed a metabolic demand that was similar to the 6MWT. A previous study9 has shown that AVG played by children with asthma led to a higher energy expenditure than achieved by aerobic testing on a treadmill.
There are few commercial computer programs designed exclusively for rehabilitation. In the vast majority of studies, and even in clinical practice, AVG originally designed for entertainment are used as a rehabilitation tool. Based on the scientific literature and the authors’ belief of its potential to provide multi-articular activity with a great variety of movement of the lower and upper limbs, the ‘Reflex Ridge’ AVG was selected for study.
The hypothesis of this study was that this game could reach high levels of intensity. The objective of the present study was to evaluate the intensity of the activity achieved by asthmatic children who played the Reflex Ridge AVG in comparison to the intensity of the activity achieved while undertaking cardiopulmonary exercise tests (CPET) on a treadmill.
MATERIALS AND METHODS
This was a cross-sectional study conducted at the Respiratory Functional Assessment Laboratory, Nove de Julho University, São Paulo, Brazil. The Ethics and Research Committee of the same institution approved the study, protocol number 907236/2014, according to resolution 466/2012 of the National Health Council. All persons responsible for minors provided informed consent for the inclusion of the minors in the study and all the children accepted the respective consent form.
Inclusion Criteria
Inclusion criteria for this study were children aged 5–11 years with a diagnosis of asthma who did not practice regular physical activity. The children were evaluated by pulmonologists.10
Exclusion Criteria
Children whose condition worsened within 30 days before testing and those who had a respiratory infection up to 2 months before testing were excluded. Additional exclusion criteria included children who had received theophylline or aminophylline and oral corticosteroids in the last 30 days; who were unable to perform any of the tests; who carried cardiac diseases of inflammatory, congenital, or ischaemic origin; and who had an infectious disease, with fever, at the time of the of the experiment.
Experimental Procedures
Screening the Asthmatic Children
Thirty-four asthmatic children were assessed and screened at Mandaqui Hospital, São Paulo, Brazil, and their parents were invited to refer them to and accompany them at the Respiratory Functional Assessment Laboratory, where the children were assessed and completed an AVG activity and a CPET. The order in which the children completed the two tests was randomised, and the two tests were performed on different days, as shown in Figure 1.
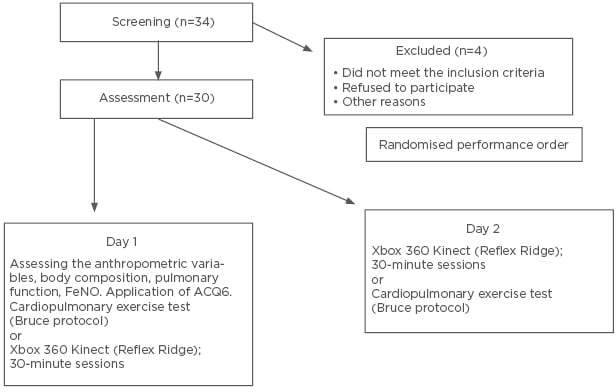
Figure 1: Flowchart showing the setup of the study.
ACQ6: Asthma Control Questionnaire 6; FeNO: fractional exhaled nitric oxide.
Anthropometric Measurements and Body Composition
All the children were individually assessed in the afternoon and anthropometric measurements, including height, weight, and tetrapolar bioimpedance11 (using a Biodynamics™ model 310, Biodynamics Corporation, Seattle, Washington, USA), were taken. The AnthroPlus software (World Health Organization [WHO]) was used to set the Z score according to the determination established by the WHO.12 The Z score was used to classify the child as obese or eutrophic (normal body weight) by keeping values between 2 and -2, depending on the Z score.
Pulmonary Function
The pulmonary function of all the children was assessed through spirometry, using the Easy One™ Air (ndd Medical Technologies, Andover, Massachusetts, USA). The spirometer was calibrated according to the Polgar and Promadhat13 reference values suited for children, prior to use in an acclimatised room. Three reproducible and technically accepted tests of forced vital capacity were recorded according to the criteria of the American Thoracic Society (ATS).14
Degree of Airway Inflammation
The degree of airway inflammation was measured through fractional exhaled nitric oxide (FeNO) and followed the ATS criteria.15 All the children performed a test using the NIOX Mino® (Circassia AB, Uppsala, Sweden) in the sitting position. This test was performed with the children exhaling and emptying their lungs as much as possible, up to the level of expiratory reserve volume, to decontaminate the respired gasses. Subsequently, a deep inspiration was recorded, and all the air was exhaled through the mouth, with constant flow through the equipment for at least 6 seconds. One minute and forty seconds later, the FeNO reading in parts per billion was recorded.16
Cardiopulmonary Exercise Test
The Bruce Test17,18 was the protocol used during the CPET and it was interrupted when the child reported or presented fatigue or when they reached the maximum heart rate (HRmax), which was set at 208 bpm minus (0.7 x age of the participant [years]).19 Blood pressure was recorded, as well as the peripheral oxygen saturation and data from the electrocardiogram.
The fatigue in the inferior limbs and the dyspnoea at effort and at rest were recorded through the modified Borg scale.20
Active Video Game
The children completed a 30-minute AVG playing session using an Xbox 360 KinectTM (Microsoft, Redmond, Washington, USA). The game used was Reflex Ridge from the Adventure Kinect video game catalogue.9
Three maximum peak flow measures were collected before and after the AVG session and CPET completion, to monitor the possible presence of exercise-induced bronchospasm (EIB); the children were kept in the standing position and used a nose clip. These measures were performed using the AssessTM (USA) equipment. Bronchospasm was characterised by a ≥20% reduction in the peak flow.21
A warm-up was performed on the treadmill for 10 minutes at a speed of 2 km/hour before the AVG session. The AVG playing section lasted 30 minutes and was composed of 10 matches (3 minutes long each) of growing effort intensity, with a mean interval of 30 seconds between matches. Increased intensity demanded a larger number of jumps, squats, and lateral displacements, as well as movements of the upper limbs.
Energy Spending
The energy spent (ES) was measured to find the MET and the calories per minute (cal/minute). This was completed using the portable SenseWear® (BodyMedia, Pittsburgh, USA) equipment algorithm v5.2 in software v.8.1, which assesses the skin temperature, as well as the galvanic skin resistance. The monitor was attached with the elastic strap around the non-dominant arm and collected data was processed in software 8.1 using measured weight and height, together with information about age, sex, and dominant arm. The movement was measured using a biaxial accelerator to calculate the energy expenditure in MET and in cal/minute.12,22
Statistical Analysis
The CPET was used as the gold standard and a comparison was made between the HRmax rate achieved during the CPET and the percentage of that HRmax rate achieved during AVG. A paired t-test was used to compare the activities. The SPSS 20.0 software was used in the analyses and the data were subjected to a normality test through visual graphic inspection and the Shapiro–Wilk test. A p value of <0.05 was considered significant.
RESULTS
Table 1 shows the data from the assessed children; 34 children started the assessment sections, but only 30 children completed the tests. Four children did not complete the protocol due to transportation difficulties reaching the evaluation site.
The children in the sample consisted mostly of moderate and severe asthmatics according to GINA criteria,10 with adequate height, percentage of body fat <20%, and FeNO levels >20 ppb (Table 1).
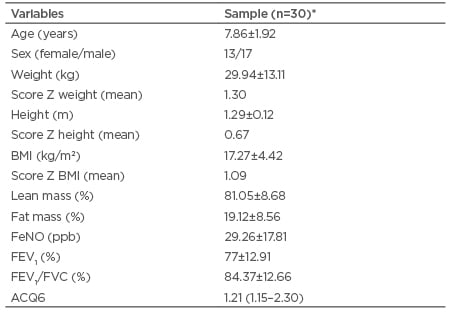
Table 1: Overall features of the 30 asthmatic children included within the sample population of this study.
*Thirty-four children started the assessment procedures but only 30 completed them. ACQ6: Asthma Control Questionnaire 6; FVC: forced vital capacity; FeNO: fractional exhaled nitric oxide; FEV1: forced expiratory volume in 1 second.
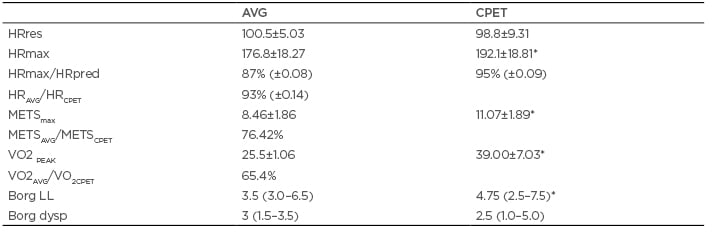
Table 2: Data comparing the ergometric test with active video game playing.
*p<0.05 paired t-test. AVG: Active videogame; BORG dysp: effort perception dyspnea; BORG LL: effort perception in lower limbs; CPET: cardiopulmonary exercise test; HRmax: maximum heart rate achieved in each activity; HRpred: predicted max heart rate for age (208-[0.7*age]); HRres: heart rate at rest; METSmax: maximum metabolic equivalent measured in each activity.
There are differences between the intensities of effort reached in CPET compared with AVG, with CPET achieving more intense activity than the AVG, but the level of effort reached when playing the AVG Reflex Ridge can still be considered moderate-to-intense.
The HRmax reached following the AVG session was 93% of that reached in the CPET, and 87% of the maximum predicted HR. An ES >6 MET is considered intense effort and >9 MET is considered a very intense effort. The perception of exertion in the lower limbs was higher during CPET compared with AVG, but there were no differences in the sensation of dyspnoea. Table 2 presents the intensity and ES data following CPET and AVG use.
The mean pre-AVG playing peak flow was 188.33±91.42 L when the mean of the greater three measures was considered, whereas the post-AVG playing peak flow was 194.66±86.70 L; thus, there was no significant difference. Just 2 out of the 30 children (6.6%) presented with a reduction >20% between the mean pre and post-physical activity peak flow during AVG playing; these children required a bronchodilator. The same children who had a reduction >20% in the peak flow in the AVG session also presented with this reduction after the CPET.
The predicted mean peak flow value of a population of children with asthma, assessed by height (cm) and recorded at sea level, would be 250.20±66.05 L according to Polgar and Promadhat.13
Discussion
According to the results presented here, the intensity of the physical activity during AVG sessions (more specifically, when playing Reflex Ridge) is high for asthmatic children. If regularly achieving this intensity is maintained for a period >8 weeks, it can lead to an increase in aerobic capacity. The children in this study reached, on average, 87% of the HRmax expected for their age group, and this was similar to the results found in previous studies,9 which have shown that 90% of expected HRmax was reached.
The literature has shown that exergames can lead to a greater energy expenditure and a more enjoyable experience than traditional physical activities, which makes children more motivated to play them. However, it is important to study different clinical conditions and age groups. McDonough et al.,23 when evaluating the intensity reached during Reflex Ridge in young adults (mean age: 23.6 years±4.1 years), found that activity intensity reached a moderate effort level, which is 3–6 MET. Traditional exercise intensity reaches an intense level >6 MET. In addition, it is thought that undergoing an interval-based physical activity is safer than continuous aerobic activity regarding the induction of bronchospasm.24
These results presented in this study are quite close to those found by Holmes et al.,25 who found individuals playing the Your Shape Xbox Kinect game achieved 86% of the HRmax achieved by individuals undergoing a CPET; however, that study recruited adults with cystic fibrosis.
AVG has been used in other populations of patients and the results appear to be promising when it comes to physical training, mainly when they are compared to results of a physical performance test. Del Corral et al.8 compared different AVG, using a Wii (Nintendo, Kyoto, Japan) device, with the 6MWT and found that some games provided an effort intensity higher than that of the 6MWT.
Another important result in the current study regards the metabolic consumption, as the children reached 8.4 MET. It is worth highlighting that peaks >6 MET are considered to be intense. Therefore, such a result is a good indicator that AVG can provide positive physiological effects in this population if carried out periodically with adequate intensity and over regular time intervals. Other studies have shown the success of AVG use, including Holmes et al.,25 who noted an exercise intensity of 6.1 MET using the Xbox Kinect in a population of adults with cystic fibrosis, and Le Gear et al.,26 who noted 3.9 MET using the Wii in adults with chronic obstructive pulmonary disease who presented with a Borg Scale of approximately 3–5.
It is possible that such results were achieved because AVG allows breaks between bouts of physical effort. Thus, video game playing is more suitable to the physiology of children, who find performing continuous and lengthy activities more difficult.27,28 Besides this, it is known that intense activities (which induce a 80–90% of HRmax response) and those with a 6–8-minute duration may trigger EIB in 40–90% of children with eosinophilic asthma (most of the children in this study were of this phenotype).25 Just 2 (6.6%) of the children in this study presented with some degree of respiratory discomfort during the time of the activity. This reinforces the safety of using AVG as a physical activity.
The activities performed on the treadmill are continuous, while video games, including the one used in this study, are interval-based. In this study, each Reflex Ridge match had a 3-minute duration, with a 30-second interval between matches, and the participants reached a mean HR of 70% of HRmax with a peak of 93%. The children usually hit this intensity in the third or fourth match out of ten in total.
According to Sidiropoulou et al.,25 regular interval-based physical activity performed by asthmatic children may reduce the risk of EIB. It is worth highlighting that the activity should be low-duration and high-intensity.
There has been growing interest in activities with AVG or exergames over recent years using both the Wii and Xbox 360. These were originally developed as entertainment systems, but this study and others like it present the potential for these systems to be therapeutic resources. However, it should be emphasised that this type of physical activity presents with certain limitations, such as the inability to establish an individual intensity for each child.
Regarding energy expenditure, Sensewear may underestimate the intensity of activities >10 MET, but it is accurate to be equivalent to calorimetry measurements at moderate activity levels as was the case in this study. The algorithm of version 8.1 of Sensewear has good applicability to evaluate energy expenditure in children, which makes it feasible for this type of evaluation.29,30 A limitation of the study was that calorimetry could have been used to record an additional measure of energy expenditure in the activity; future studies may consider this possibility.
CONCLUSION
These results show that high-intensity physical activities using AVG can ensure an exercise intensity similar to that of exercises performed on ergonomic treadmill to be drawn. AVG playing can be considered a safe, motivating, and efficient treatment modality for asthmatic children.





