Presenter: Junichi Ishii
Fujita Health University School of Medicine, Toyoake, Japan
Disclosure: The author has declared no conflicts of interest.
Acknowledgements: Writing assistance was provided by Dr Julia Duffey, Manifold Medical Communications, Derbyshire, UK.
Support: The publication of this article was funded by Siemens Healthineers via an educational grant.
Citation: EMJ Cardiol. 2020;8[1]:42-44.
Meeting Summary:
Acute myocardial infarction (AMI) is a common and life-threating condition. Approximately 10% of all emergency department (ED) consultations are for suspected AMI, which places a large burden on healthcare systems. Because of the high levels of morbidity and mortality, rapid diagnosis and treatment is crucial.1-4 The European Society of Cardiology (ESC) suggests the use of the 0-hour/1-hour algorithm for rapid ‘rule-out’ and ‘rule-in’ of non-ST-segment-elevation myocardial infarction (NSTEMI) by adopting high-sensitivity cardiac troponin I (hsTnI) assays.2,5 However, there are limited data regarding the use of this algorithm in Asian populations.
Prospective Validation of 0-Hour/1-Hour Algorithm Using High-Sensitivity Cardiac Troponin I in Japanese Patients Presenting to the Emergency Department
In 2015, the ESC recommended the use of the 0-hour/1-hour algorithm as an alternative to the 0-hour/3-hour algorithm, to rule-in or rule-out AMI based on hsTnI assays for patients presenting with suspected non-ST-elevation acute coronary syndromes in the emergency room. Several studies demonstrated that hsTnI at presentation and after 1 hour had similar diagnostic accuracy compared to the 3-hour algorithm. It was suggested that using the hsTnI 0-hour/1-hour algorithm may improve the time to diagnosis and treatment. Furthermore, the use of this algorithm may also reduce the length of stay in the ED for patients in whom NSTEMI has been excluded. Multiple assays measuring hsTnI exist. Each assay varies in diagnostic accuracy and cut-off levels. Furthermore, limited data are available that have validated the 0-hour/1-hour algorithm using hsTnI in Asian populations.
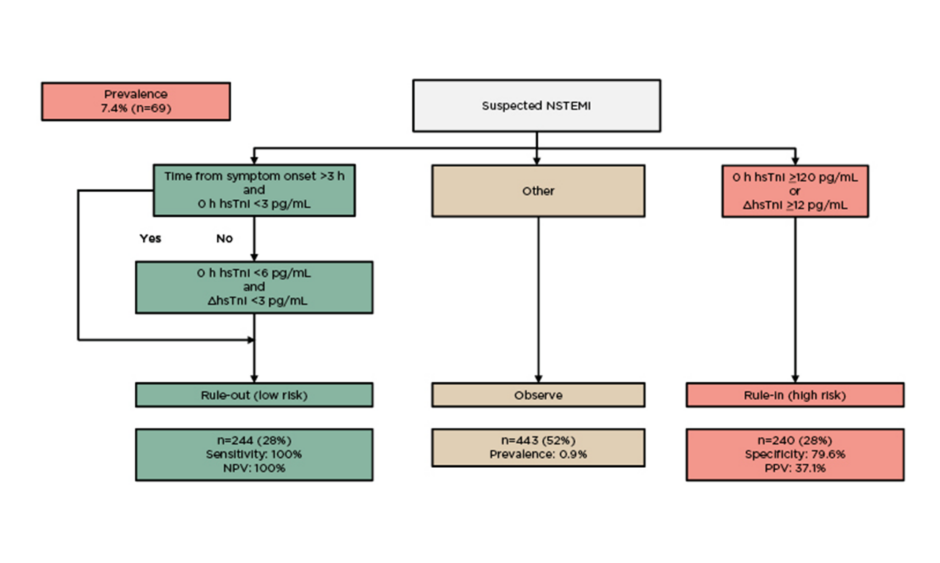
This single-centre, prospective study validated the 0-hour/1-hour algorithm using hsTnI in Japanese patients (median age: >20 years) presenting to the ED.6 The hsTnI concentration was measured using the ADVIA Centaur® High-Sensitivity Troponin I Assay (Siemens Healthineers, Erlangen, Germany) at presentation and after 1 hour. Patients were divided into three groups according to the algorithm:
- Rule-out (low risk) group: hsTnI <3 ng/L if chest pain onset was >3 hours or <6 ng/L and Δ1 hour <3 ng/L.
- Rule-in (high risk) group: hsTnI ≥120 ng/L or Δ1 hour ≥12 ng/L.
- ‘Observe’ group: all other patients.
Based on the fourth universal definition of myocardial infarction,7 the final diagnosis was adjudicated by two independent cardiologists using all available information, including coronary angiography, coronary CT, and follow-up data. The safety of rule-out was determined by the negative predictive value for NSTEMI. The accuracy of rule-in was determined by the positive predictive value. The overall efficacy of the 0-hour/1-hour algorithm and the ADVIA Centaur High-Sensitivity Troponin I Assay was defined as the proportion of patients triaged towards rule-out or rule-in within 1 hour.
A total of 754 Japanese patients (mean age: 71.1 years; male: n=395), with symptoms suggestive of NSTEMI with serial hsTnI testing, were included in this investigation. The most common comorbidities were hypertension (59%), followed by dyslipidaemia (33%) and diabetes (24%). For the patients with AMI (n=69), the 0-hour median hsTnI was 116 pg/mL (interquartile range [IQR]: 24.2−1,111.0) and 1-hour hsTnI was 362 pg/mL (IQR: 87.5−2,129.0). For the patients without AMI (n=858), the 0-hour hsTnI was 13.0 pg/mL (IQR: 5.0−48.0) and 1-hour hsTnI was 13.5 pg/mL (IQR: 5.4−56.1).
The prevalence of NSTEMI was 7.4% (Figure 1). The safety (negative predictive value) of the 0-hour/1-hour algorithm using hsTnI was 100%, and 28% of patients could be ruled-out.
Figure 1: Findings of the first clinical validation of the of 0-hour/1-hour algorithm using high-sensitivity cardiac troponin I in Japanese patients presenting to the emergency department.
ED: emergency department; h: hours; hsTnI: high-sensitivity cardiac troponin I; NPV: negative predictive value; NSTEMI: non-ST-segment-elevation myocardial infarction; PPV: positive predictive value.
Adapted with permission from Ohtake et al.6
First presented during ESC Congress 2020 – The Digital Experience
The proportion of patients who could be ruled in was 28%. The accuracy for the rule-in group, determined by the positive predictive value, was 37.1% and the specificity was 79.6%. These data show that the 0-hour/1-hour algorithm using the ADVIA Centaur High-Sensitivity Troponin I Assay is a safe and effective tool for triaging Japanese patients presenting to the ED with suspected NSTEMI. The diagnostic accuracy and sensitivity of the 0-hour/1-hour algorithm using this assay is high and comparable with other well-established methods.1 The use of this algorithm and assay supports the triage of patients within 1 hour of ED presentation for the majority of individuals, reducing the time to treatment initiation and the length of stay in the ED.
During the ESC Congress 2020, new non-ST-segment-elevation acute coronary syndrome guidelines were introduced.5 Validation of the 0-hour/1-hour algorithm with a Japanese population aligns with the latest guidelines and confirms the Advantageous Predictors of Acute Coronary Syndromes Evaluation (APACE) algorithm validation published in 2018.1






