Abstract
The diagnosis of Pneumocystis jirovecii pneumonia (PJP) in immunocompromised patients remains challenging despite the use of conventional staining techniques in bronchoalveolar lavage samples. Quantitative PCR (qPCR) has demonstrated improved diagnostic accuracy compared with traditional methods. This scoping review evaluated the diagnostic validity of conventional stains versus qPCR for PJP diagnosis in immunocompromised patients. Comprehensive searches of MEDLINE, PubMed, Cochrane Library, and CINAHL databases were conducted between April–October 2025 for studies published from 1985 onwards. A reproducible search strategy using predefined Medical Subject Headings terms and eligibility criteria was applied. Of 856 identified studies, eight met inclusion criteria for final analysis. Methodological quality was assessed using Joanna Briggs Institute critical appraisal tools. Most included studies originated from high-income countries and focused on adult populations, whereas paediatric and developing-world data were limited. Gomori methenamine silver staining showed lower sensitivity and specificity than immunofluorescence assay, while qPCR consistently demonstrated superior diagnostic performance. However, findings should be interpreted cautiously because of limited study numbers and methodological heterogeneity. Further multicentre studies are required to validate the clinical utility of qPCR in PJP diagnosis.
Key Points
1. This scoping review highlights that diagnosing Pneumocystis jirovecii pneumonia (PJP) in immunocompromised patients remains difficult, particularly in low-resource settings, due to the limited sensitivity of conventional staining methods and lack of standardised diagnostic protocols across clinical laboratories.
2. Quantitative PCR testing on bronchoalveolar lavage samples demonstrates markedly higher sensitivity and specificity than traditional staining techniques, supporting its potential role as a gold-standard diagnostic method for PJP.
3. The review identifies major research and practice gaps, particularly in paediatric and developing-world data, emphasising the need for international collaboration to validate PCR-based diagnostics and guide evidence-based clinical and policy decision-making for PJP management.
INTRODUCTION
Pneumocystis jirovecii pneumonia (PJP) is a severe opportunistic infection caused by the fungal organism P. jirovecii.¹ It represents a significant cause of morbidity and mortality among immunocompromised patients, both with and without AIDS.² Bronchoalveolar lavage (BAL), first introduced in 1974 for diagnosing respiratory diseases such as sarcoidosis and idiopathic pulmonary fibrosis,³ has since become a valuable diagnostic tool. BAL enables the identification of infectious agents in individuals who are immunocompromised through cellular analysis and specific staining techniques.⁴ During the AIDS epidemic of the 1980s, BAL was increasingly utilised to diagnose Pneumocystis carinii pneumonia (PCP)/PJP.⁵ By the mid-1990s, the Wright–Giemsa (WG) and Gomori methenamine silver (GMS) stains were established as gold-standard diagnostic techniques for PCP/PJP via BAL.⁶ BAL provides a higher diagnostic yield compared to induced sputum and lung biopsy.⁷ Immunofluorescence assay (IFA) has been demonstrated to be superior to conventional staining methods.⁸ Although quantitative PCR (qPCR) is a promising molecular diagnostic approach, it has not yet been fully incorporated into formal diagnostic guidelines.⁹ Traditional microscopic stains often fail to detect PJP in a substantial number of cases,¹⁰ leaving many patients undiagnosed and at increased risk of mortality. This has caused a huge gap in regard to diagnosing PJP in suspected cases. Those undiagnosed patients of suspected PJP become at high risk of mortality and a point of concern for clinicians as well. The use of qPCR on BAL specimens offers improved diagnostic accuracy, particularly in patients who test negative by conventional methods.⁷ This approach may aid clinicians and policymakers in establishing standardised diagnostic protocols. Therefore, the objective of this scoping review was to analyse previous and recent literature to evaluate the different gaps and compare sensitivity and specificity of immunofluorescence and GMS stains, as contrasted to qPCR, through BAL procedure for diagnosis of PJP in immunocompromised patients.
METHODS
The BAL procedure requires specialised expertise and advanced medical equipment, which may not be readily available in resource-limited settings. In immunocompromised paediatric patients, clinicians often avoid BAL unless strongly indicated because of procedural concerns and limited available evidence.⁴ To evaluate the validity of qPCR in BAL samples for PJP diagnosis, this scoping review was conducted to identify research gaps not comprehensively addressed in previous reviews. The review followed the five-stage methodological framework proposed by Arksey and O’Malley:¹¹ 1) identifying the research question; 2) identifying relevant studies; 3) selecting studies for detailed analysis; 4) charting the data; and 5) collating, summarising, and reporting the results.
The literature search included studies published between 1985–October 2025. Database searches were conducted between 1st April 2025–10th October 2025. The databases consulted were PubMed, MEDLINE, CINAHL, and the Cochrane Library to ensure comprehensive coverage of published literature. A transparent and reproducible search strategy was developed using combinations of Medical Subject Headings terms, keywords, and Boolean operators. The following search terms were used in PubMed: “bronchoalveolar lavage” and diagnosis or detection, and “Pneumocystis jirovecii pneumonia” or “Pneumocystis carinii pneumonia” or PCP. Similar search strategies were adapted for MEDLINE, CINAHL, and the Cochrane Library using database-specific indexing terms. No restrictions were initially applied regarding publication date or study design during the database search stage. Grey literature was not included.
Titles and abstracts were independently screened by two reviewers. Full-text articles considered potentially eligible were subsequently reviewed using the same strategy. Any disagreements between reviewers were resolved through discussion and consensus. Studies selected for review included RCTs, cohort studies, observational studies, and controlled studies.
The inclusion criteria were: 1) studies involving immunocompromised adult patients; 2) studies evaluating PCP/PJP diagnosis using BAL samples; 3) studies published in English; 4) studies comparing PCR-based techniques with conventional staining methods such as GMS, WG, or IFA; and 5) studies reporting at least one relevant diagnostic outcome including sensitivity or specificity. Exclusion criteria included animal studies, cell-based studies, duplicate studies, case reports, reviews, conference posters, studies with incomplete data, and non-English publications.
The identified studies were downloaded and duplicates were removed. Two reviewers independently screened titles, abstracts, and full texts according to predefined inclusion and exclusion criteria. Data extraction was performed independently using a standardised checklist. Extracted data included author name, country of study, study design, population size, demographic characteristics, diagnostic methods, sensitivity, specificity, and major outcomes. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) framework was used to guide study selection and reporting.12
To strengthen methodological rigour, a structured quality appraisal of included studies was additionally performed using the Joanna Briggs Institute (JBI) critical appraisal tools appropriate for each study design.13 The appraisal evaluated participant selection, measurement reliability, outcome assessment, confounding factors, and statistical analysis. Studies were not excluded based on quality assessment, because the primary aim of this scoping review was to map the available evidence; however, methodological limitations were considered during interpretation of findings.
The outcomes for this scoping review were: 1) sensitivity and specificity of traditional staining methods (GMS, WG, and IFA) used in the diagnosis of PJP through BAL; 2) sensitivity and specificity of qPCR compared with with the gold-standard methods; and 3) epidemiological and demographic factors influencing diagnostic performance. All outcomes were summarised descriptively using tables and narrative synthesis.
RESULTS
A total of 856 studies were identified through database searches (Figure 1). After removal of duplicates, 690 studies remained for eligibility screening. Following title and abstract screening, 664 studies were excluded and 26 studies underwent full-text review. After detailed assessment against the inclusion and exclusion criteria, eight studies were retained for final analysis.
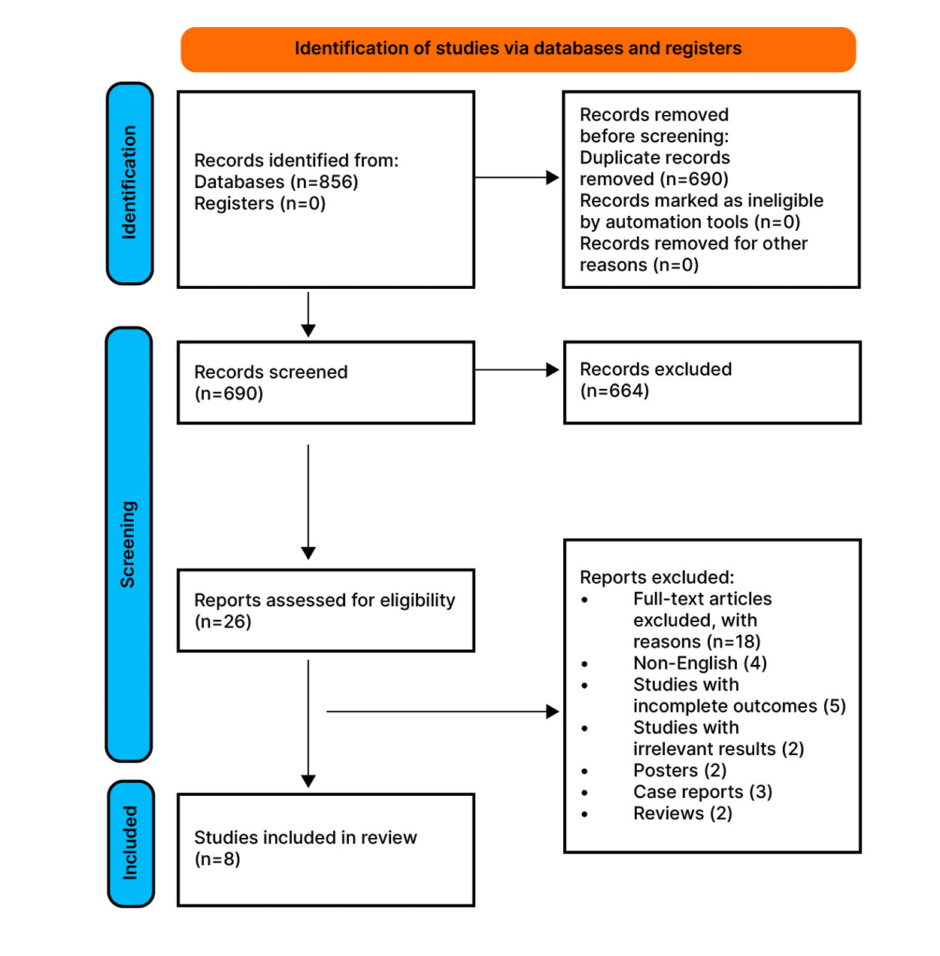
Figure 1: PRISMA flow diagram showing selection of studies.
Quality Appraisal of Included Studies
Structured methodological appraisal using the JBI critical appraisal tools demonstrated that most included studies had moderate methodological quality. Common strengths included clearly defined diagnostic objectives and appropriate use of BAL specimens for microbiological assessment. However, several studies demonstrated limitations, including small sample sizes, single-centre designs, retrospective data collection, and variability in PCR threshold values and comparator staining methods. In addition, heterogeneity in patient populations and laboratory protocols limited direct comparison across studies. These methodological limitations were considered during interpretation of the findings.
Sensitivity and Specificity Among Gold-Standard Stains
During the 1990s, the WG and GMS stains were considered the gold standard for the diagnosis of PJP using BAL samples.6 Subsequently, the IFA was added and recognised as an additional gold-standard technique.14 Several studies published between 1990–2020 evaluated the clinical efficacy of IFA, Giemsa, and GMS stains in diagnosing PJP in immunocompromised patients (Table 1).15-22 Among the eight studies included, three examined the diagnostic performance of qPCR compared with traditional stains such as IFA and GMS.15-20 However, three studies investigated the qPCR cycle threshold in comparison with IFA for diagnosing PJP in immunosuppressed individuals.18-20 In addition, two studies compared the sensitivity and specificity of GMS and direct staining methods with PCR using BAL samples, demonstrating noteworthy diagnostic outcomes.21,22
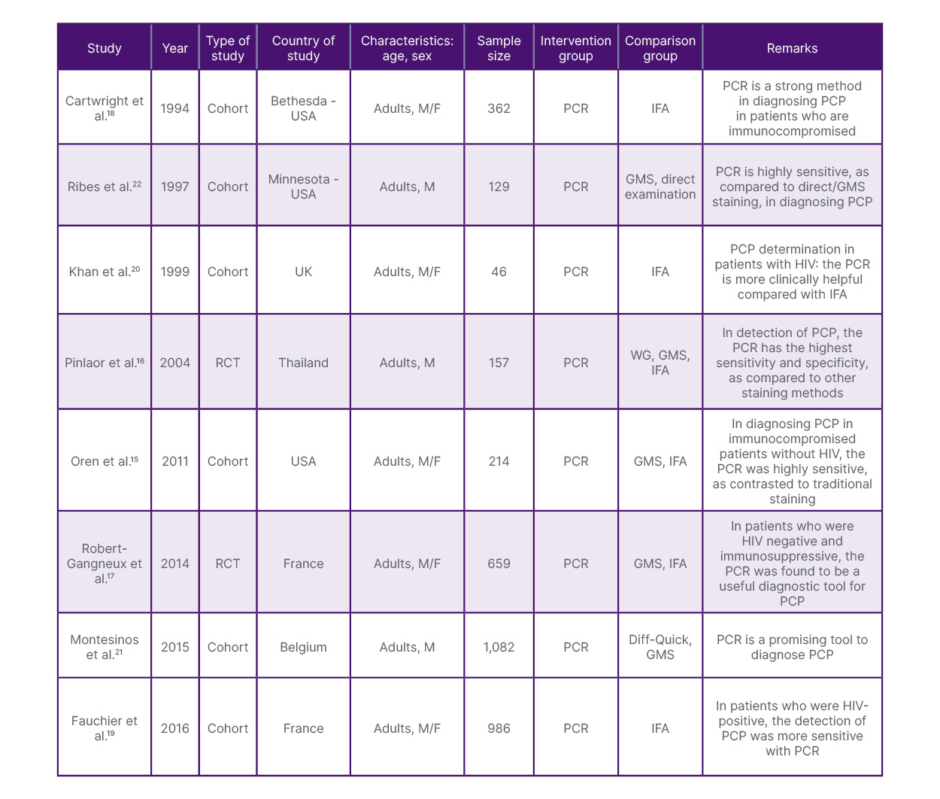
Table 1: Characteristics of studies included in scoping review.15-22
F: Female; GMS: Gomori methenamine silver; IFA: Immunofluorescence assay; M: Male; PCP: Pneumocystis carinii pneumonia; WG: Wright–Giemsa.
Sensitivity and Specificity of PCR as Compared to Traditional Stains
Across most included studies, qPCR demonstrated higher sensitivity and specificity than conventional staining techniques, with consistently high negative predictive values (Table 2).15-22 Montesinos et al.21 and Ribes et al.22 reported GMS sensitivities of 45% and 86%, and specificities of 95% and 75%, respectively. In comparison, PCR demonstrated sensitivities of 65% and 85%, and specificities approaching 100%. Cartwright et al.,18 Fauchier et al.,19 and other investigators described IFA sensitivities ranging from 66–100% and specificities from 92–100%, whereas PCR generally demonstrated superior diagnostic performance. Collectively, these findings indicate that PCR provides higher diagnostic accuracy for PCP in immunocompromised patients, particularly in cases where conventional staining methods fail to detect infection.
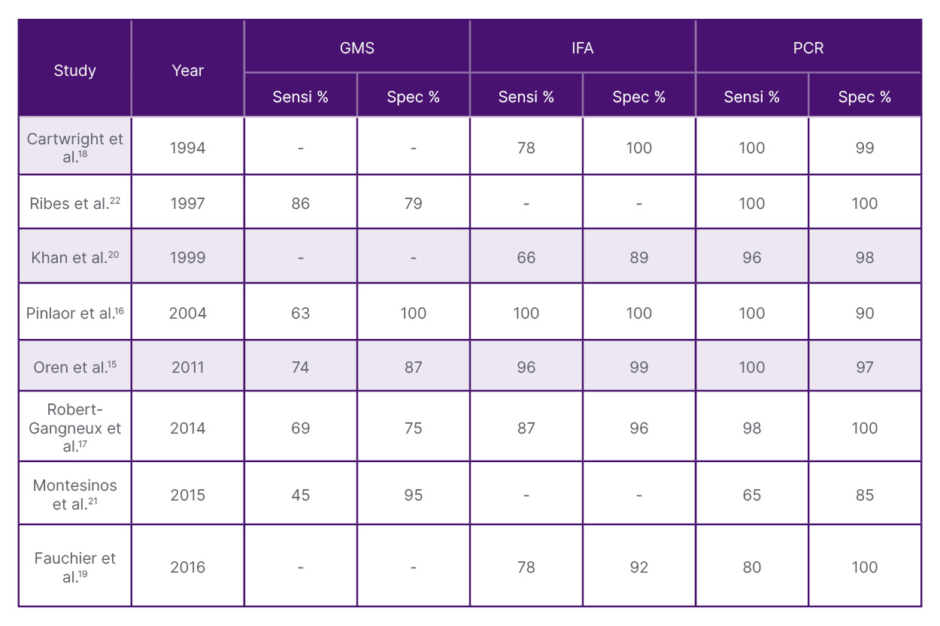
Table 2: Sensitivity and specificity of traditional stains versus PCR.15-22
GMS: Gomori methenamine silver; IFA: immunofluorescence assay; Sensi: sensitivity; Spec: specificity.
However, the interpretation of PCR results requires clinical correlation. PCR-based techniques may detect low fungal burdens or airway colonisation in immunocompromised individuals without active disease. Consequently, positive PCR findings should be interpreted alongside clinical presentation, radiological findings, fungal burden thresholds, and host immune status. Variation in PCR cycle threshold values and lack of universally standardised cut-offs across laboratories may also affect diagnostic interpretation and comparability between studies.
Epidemiological andOther Characteristics
Following the removal of duplicates, 690 studies were screened. Of these, 26 were selected for full-text review, and eight met the inclusion criteria for this scoping review (Figure 1[/hl]). The included studies originated primarily from high-income countries, including the USA, UK, Belgium, France, Thailand, and other European centres. Limited statistical data were identified from Africa or Asia, highlighting a potential global evidence gap and possible under-representation of the true burden of PJP in resource-limited settings. Most studies included both male and female participants, although several studies predominantly involved male populations. Only a limited number of studies evaluated paediatric patients, whereas most focused on immunocompromised adult populations undergoing BAL for suspected PJP diagnosis.
DISCUSSION
In this scoping review, qPCR performed on BAL samples generally demonstrated higher sensitivity and specificity than conventional staining methods for diagnosing PJP in immunocompromised patients. Nevertheless, important methodological and epidemiological gaps remain within the available literature. Most included studies originated from developed countries such as the UK, USA, France, Germany, and Japan, whereas limited evidence was available from Africa and many Asian regions. This disparity may reflect differences in access to specialised laboratory facilities, bronchoscopy services, molecular diagnostic technologies, and research infrastructure. Consequently, the true epidemiological burden of PJP in low-resource settings may be under-recognised.
A further limitation identified in the literature was the scarcity of paediatric studies. Due to the invasive nature of BAL and limited available evidence in children, clinicians may be reluctant to perform BAL procedures in paediatric patients unless strongly indicated. Thus, the accuracy of cases in children, as well as the mortality rate, remains unclear. Due to restricted data, the use of BAL in children is limited, and it remains uncertain whether PCR or traditional staining methods provide better diagnostic yield. To fulfill these gaps, the developed nations should come forward and support funds in order to provide suitable equipment, training for healthcare professionals, and encouragement for researchers in resource-limited settings to conduct and publish paediatric studies.
Several studies demonstrated that traditional staining methods such as GMS and IFA retain clinical utility in diagnosing PJP.17,19,22 However, Pinlaor et al.16 reported that both GMS and IFA achieved 100% specificity, suggesting that these techniques can be used for screening asymptomatic patients with PCP. However, they also noted that PCR and IFA are more costly and time-consuming. Conversely, Oren et al.15 and Robert-Gangneux et al.17 observed that the sensitivity and specificity of GMS were lower than those of IFA, with IFA demonstrating superior diagnostic accuracy (Table 2).15-22 Montesinos et al.21 found that GMS had the lowest sensitivity and specificity among the evaluated methods. Collectively, these findings suggest that conventional staining methods remain valuable but may fail to identify cases with low fungal burden.
Most investigators comparing qPCR with conventional staining techniques reported superior sensitivity and negative predictive value for PCR-based assays. Fauchier et al.19 and Khan et al.20 evaluated the diagnostic yield of PCR performed on BAL samples from patients who remained undiagnosed using IFA.19,20 They concluded that the sensitivity and specificity of IFA were 66% and 89%, and 78% and 92%, respectively, compared with PCR, which achieved nearly 100% in both measures. However, Cartwright et al.18 reported equal sensitivity and specificity between IFA and PCR. Montesinos et al.21 assessed the clinical value of PCR testing in BAL samples and found sensitivities of 45% for GMS and 65% for PCR, and specificities of 95% and 85%, respectively. Based on the evaluation of these trials, the clinical validation of PCR is well established for diagnosing PCP in immunocompromised patients. However, an important limitation of PCR is its inability to consistently differentiate active infection from colonisation. P. jirovecii colonisation may occur in patients who are immunocompromised without overt clinical disease, particularly in individuals with chronic lung disease or low organism burden. Therefore, PCR positivity alone should not be interpreted as definitive evidence of active PJP.
Interpretation of PCR findings should incorporate the overall clinical context, including symptoms, radiological imaging, host immune status, and fungal burden indicators such as cycle threshold values. In addition, variability in PCR assays, laboratory protocols, and threshold cut-offs across institutions limits standardisation, and may influence diagnostic accuracy. Consequently, although qPCR appears highly sensitive, further multicentre prospective studies are required before universal adoption as a sole reference standard can be recommended.
This scoping review has several limitations. Although two independent reviewers conducted study screening and selection, the possibility of selection bias cannot be completely excluded.23 Only English-language studies were included, potentially introducing geographic and language bias. Furthermore, the number of included studies was limited, and considerable heterogeneity existed regarding study design, patient populations, comparator methods, and PCR protocols. Formal meta-analysis was therefore not appropriate. Additionally, alternative diagnostic methods such as May–Grünwald–Giemsa and Fungifluor staining were not evaluated in this review. These methods may demonstrate comparable sensitivity and specificity to qPCR, and their exclusion may have limited the comprehensiveness of this review.
CONCLUSION
This scoping review suggests that qPCR performed on BAL samples demonstrates higher sensitivity and specificity than conventional staining methods for diagnosing PJP in immunocompromised patients. However, findings should be interpreted cautiously because of limited study numbers, methodological heterogeneity, and under-representation of paediatric and low-resource populations. Although qPCR offers important diagnostic advantages, it may not reliably distinguish colonisation from active infection. Therefore, PCR results should be interpreted alongside clinical and radiological findings. Further multicentre studies are needed to standardise PCR thresholds, evaluate cost-effectiveness, and guide integration of molecular diagnostics into future clinical guidelines.






