Abstract
Disseminated tuberculosis represents hematogenous spread of Mycobacterium tuberculosis involving multiple organ systems. Although commonly associated with immunosuppression, it can occasionally occur in immunocompetent individuals and pose diagnostic challenges. The authors report an immunocompetent adult who presented with constitutional symptoms and respiratory complaints. Imaging revealed pleural effusion with hepatic and splenic involvement, raising an initial differential diagnosis of disseminated infection or malignancy. Microbiological evaluation demonstrated positivity for M. tuberculosis in cartridge-based nucleic acid amplification testing from both sputum and gastric aspirate, confirming active tuberculosis with multisystem involvement. The patient was HIV-negative and had no underlying comorbidities or immunosuppressive conditions. Antitubercular therapy was initiated with significant clinical and radiological improvement.
Key Points
1. Disseminated tuberculosis can occur in immunocompetent individuals and should be considered in patients presenting with prolonged constitutional symptoms and multisystem involvement, even in the absence of classical risk factors such as HIV infection, diabetes, or immunosuppressive therapy.
2. Hepatic and splenic involvement in tuberculosis is uncommon and often mimics malignancy or other systemic infections on imaging. Awareness of these atypical manifestations is crucial to avoid diagnostic delay and unnecessary invasive investigations.
3. Microbiological confirmation using rapid molecular tests, such as cartridge-based nucleic acid amplification tests, from multiple accessible sites, including sputum and gastric aspirate, can establish the diagnosis of disseminated tuberculosis and enable early initiation of antitubercular therapy, leading to favourable clinical and radiological outcomes.
INTRODUCTION
Tuberculosis remains a major global health problem, with extrapulmonary manifestations accounting for a significant proportion of cases, particularly in endemic regions. Disseminated tuberculosis results from lymphohematogenous spread of Mycobacterium tuberculosis and is characterised by involvement of two or more non-contiguous organ systems.1 It is most reported in individuals with impaired immunity, including those with HIV infection, malignancy, chronic kidney disease, or prolonged immunosuppressive therapy. However, disseminated tuberculosis can also occur in immunocompetent individuals, where it often poses a diagnostic challenge due to its nonspecific clinical presentation and ability to mimic malignancy or other systemic infections. In such patients, delayed diagnosis is common and may contribute to extensive multisystem involvement. Hepatic and splenic tuberculosis, in particular, are uncommon and frequently under-recognised, as symptoms are subtle and imaging findings may resemble metastatic disease or pyogenic abscesses.2,3
Microbiological confirmation remains the cornerstone of diagnosis, but obtaining tissue samples from extrapulmonary sites may be invasive or technically difficult. The availability of rapid molecular diagnostic techniques, such as cartridge-based nucleic acid amplification tests (CBNAAT), has significantly improved diagnostic yield and allows early initiation of therapy. The authors report a case of disseminated tuberculosis with pleural, hepatic, and splenic involvement in an immunocompetent adult male, emphasising the role of microbiological confirmation from multiple sites and the importance of maintaining a high index of suspicion even in the absence of immunosuppression.
CASE DESCRIPTION
Patient Information
A 42-year-old male with no known comorbidities presented with low-grade fever for 2 months, cough for 1.5 months, progressive breathlessness, generalised weakness, loss of appetite, and weight loss. There was no prior history of tuberculosis, diabetes, immunosuppressive drug use, or high-risk behaviour. Relevant investigations and clinical parameters supporting immunocompetent status are summarised in Table 1.
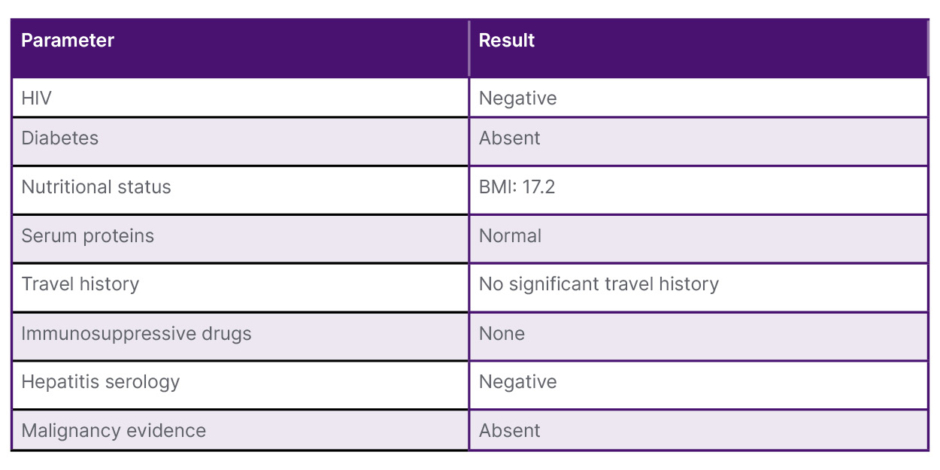
Table 1: Clinical and laboratory parameters supporting the patient’s immunocompetent status.
Clinical Findings
On examination, the patient was ill-built and poorly nourished. He was pale, with no icterus or cyanosis. Vital signs showed a pulse rate of 90 /min, blood pressure 90/60 mmHg, respiratory rate 26 /min, and oxygen saturation 98% on room air. Respiratory examination revealed reduced breath sounds on the right side with bilateral crepitations. Abdominal examination showed hepatosplenomegaly with mild ascites.
Diagnostic Assessment
Laboratory investigations revealed anaemia, hypoproteinaemia, and hyponatraemia, which was corrected during hospital stay. HIV serology was negative. Chest radiograph demonstrated bilateral nodular opacities with right pleural effusion (Figure 1). Ultrasound chest showed loculated right pleural collection with septations suggestive of empyema and mild left pleural effusion. Contrast-enhanced CT of the thorax and upper abdomen revealed right pleural effusion with enhancing pleura (split pleura sign), bilateral pulmonary nodules with a tree-in-bud pattern, necrotic mediastinal and abdominal lymph nodes, hepatomegaly with multiple hypodense lesions suggestive of microabscesses, splenic granulomas, and mild ascites, consistent with disseminated tuberculosis (Figure 2). The patient was severely malnourished and clinically frail at presentation. Following multidisciplinary discussion with the departments of General Surgery and Gastroenterology, a decision was made to initiate antitubercular therapy and monitor for early clinical response rather than proceed immediately with invasive diagnostic procedures. It was planned that invasive tissue sampling would be considered if there was no significant clinical improvement after 1 month of therapy. As the patient subsequently demonstrated clear clinical improvement on antitubercular treatment, invasive procedures were deferred.
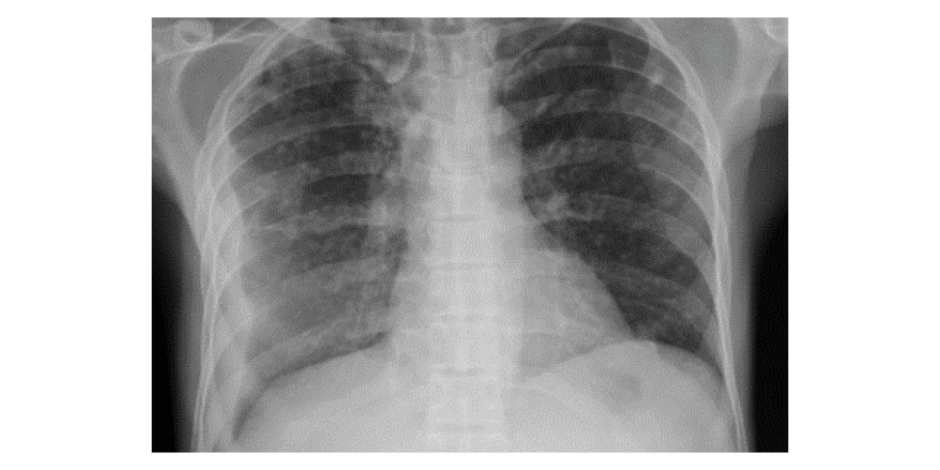
Figure 1: Chest radiograph (posteroanterior view) showing bilateral nodular opacities with evidence of a right-sided pleural effusion.
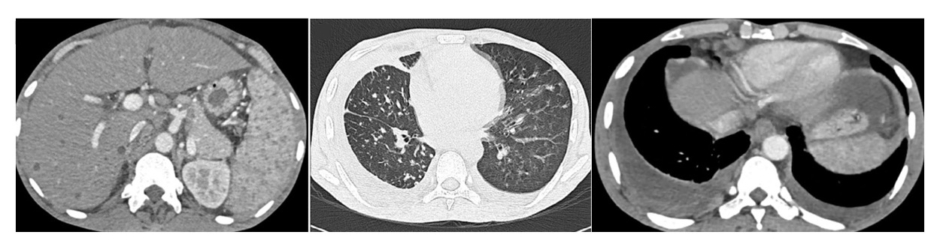
Figure 2: Thoracoabdominal CT findings suggestive of disseminated tuberculosis.
Contrast-enhanced CT of the thorax and upper abdomen demonstrating right-sided pleural effusion with thickened enhancing pleura (split pleura sign), diffuse bilateral pulmonary nodules with a tree-in-bud pattern, necrotic mediastinal and abdominal lymphadenopathy, hepatomegaly with multiple hypodense lesions suggestive of microabscesses, splenic granulomas, and mild ascites, consistent with disseminated tuberculosis.
Due to poor oral intake, the patient was on Ryle’s tube feeding. CBNAAT testing of sputum and gastric aspirate detected M. tuberculosis, confirming active tuberculosis.
Therapeutic Intervention
Antitubercular therapy was initiated as per national guidelines. Cardiothoracic surgical consultation was obtained for evaluation of the loculated pleural empyema. However, the patient was considered medically unfit for invasive intervention because of severe malnutrition, low BMI, poor general condition, and extensive disseminated disease. Pleural drainage was technically difficult due to dense septations, and surgical intervention was therefore deferred. Following initiation of antitubercular therapy, the patient demonstrated progressive clinical and radiological improvement, and conservative management with close follow-up was continued.
Follow-Up and Outcomes
The patient demonstrated progressive symptomatic improvement after initiation of therapy. Follow-up chest radiograph after 3 months demonstrated interval radiological improvement, although image quality was limited because the radiograph was performed outside the authors’ institution and the original digital image was unavailable. Follow-up abdominal CT imaging could not be performed because of financial constraints. However, ultrasound examination of the abdomen performed after 3 months at an outside facility demonstrated resolving hepatic and splenic lesions, supporting interval improvement following antitubercular therapy. The patient continues antitubercular therapy with regular follow-up.
DISCUSSION
Disseminated tuberculosis results from hematogenous spread of M. tuberculosis and is traditionally associated with immunocompromised states such as HIV infection, malignancy, or prolonged immunosuppressive therapy.2,3 However, disseminated disease can also occur in immunocompetent individuals, particularly in tuberculosis-endemic regions, where delayed diagnosis and high bacillary burden may contribute to multisystem involvement.4
The present case demonstrates disseminated tuberculosis with pleural, hepatic, and splenic involvement in an immunocompetent adult. While pleural tuberculosis is a common extrapulmonary manifestation, hepatic and splenic involvement are relatively uncommon and often underdiagnosed due to their nonspecific clinical presentation.5
Hepatosplenic tuberculosis may present as focal hypodense lesions or diffuse organ enlargement on imaging, frequently mimicking metastatic malignancy, lymphoma, or pyogenic abscesses, thereby posing a diagnostic challenge.6,7
Radiologically, hepatosplenic tuberculosis may mimic lymphoma or metastatic disease. However, the presence of concomitant pulmonary findings, necrotic lymphadenopathy, constitutional symptoms, splenic microabscesses, and microbiological confirmation by CBNAAT favoured disseminated tuberculosis in the present case. Lymphoma typically presents with homogeneous lymphadenopathy and splenomegaly, whereas metastases are usually associated with a known primary malignancy.
A key strength of this case is microbiological confirmation from two independent sites. Positivity of CBNAAT from both sputum and gastric aspirate provided strong evidence of active mycobacterial infection and supported the diagnosis of disseminated tuberculosis. Molecular diagnostic tests have significantly improved the rapid detection of tuberculosis and are recommended by the WHO for both pulmonary and extrapulmonary samples.8 In the presence of compatible clinical and radiological findings, microbiological confirmation from multiple sites may obviate the need for invasive tissue biopsy, particularly when procedural risks are high or resources are limited.9
The authors acknowledge that the absence of mycobacterial culture positivity and extended phenotypic drug susceptibility testing is a limitation of this case. Although mycobacterial culture remains the reference standard for confirmation and comprehensive drug-resistance assessment, culture in the authors’ patient was negative. However, CBNAAT performed on both sputum and gastric aspirate detected M. tuberculosis with no evidence of rifampicin resistance. In the setting of compatible clinical and radiological findings, these results strongly supported the diagnosis of disseminated tuberculosis and guided initiation of antitubercular therapy. Nevertheless, the inability to perform extended drug susceptibility testing should be recognised, particularly given the importance of drug-resistance evaluation in disseminated tuberculosis.
Although disseminated tuberculosis is more frequently reported in immunocompromised hosts, several studies have documented its occurrence in immunocompetent individuals.4,10 Proposed mechanisms include delayed diagnosis, high mycobacterial load, and host genetic susceptibility. Importantly, immunocompetence should be carefully documented. In this patient, HIV testing was negative and there was no history of diabetes, chronic kidney disease, malignancy, or immunosuppressive drug use.
The authors also acknowledge imaging-related limitations in this report. The follow-up chest radiograph available for publication was of suboptimal quality because the study was performed outside of the authors’ institution. In addition, follow-up abdominal CT imaging could not be obtained because of financial constraints, although interval improvement in hepatosplenic lesions was demonstrated on follow-up ultrasonography.
This case highlights several important clinical lessons. Disseminated tuberculosis should remain a diagnostic consideration in patients presenting with constitutional symptoms and multisystem involvement, even in the absence of overt immunosuppression. Microbiological evaluation from multiple accessible sites, including gastric aspirate, can enhance diagnostic yield when sputum examination alone may be insufficient.8,11 Early diagnosis and prompt initiation of antitubercular therapy are essential to reduce morbidity and ensure favourable outcomes.
CONCLUSION
Disseminated tuberculosis can occur in immunocompetent individuals and may present with multisystem involvement that mimics malignancy or other systemic diseases. Microbiological confirmation from multiple accessible sites can establish the diagnosis and may obviate the need for invasive procedures. A high index of suspicion and early initiation of antitubercular therapy are essential to ensure favourable outcomes.






