
Abstract
Introduction: Magnetic resonance cholangiopancreatography (MRCP) is an important diagnostic tool in evaluating patients with biliary laboratory abnormalities after orthotopic liver transplant (OLT) to determine the need for more invasive procedures, such as endoscopic retrograde cholangiopancreatography (ERCP), which can deliver therapeutic interventions. The aim of this study was to determine the diagnostic accuracy of MRCP findings using ERCP as the gold standard in a group of post-OLT patients.
Methods: A retrospective review of 273 patients who underwent OLT at the University of South Florida and Tampa General Hospital, Tampa, Florida, USA, from January 2012–April 2015 was performed. A total of 52 patients who had a MRCP and underwent a subsequent ERCP were studied. Presence of anastomotic stricture, common bile duct dilation >0.7 mm, bile leak, stone, intrahepatic stricture, or extrahepatic stricture on either modality was recorded. SPSS statistical analysis software (version 22 for Windows, SPSS Inc., Chicago, Illinois, USA) was used to calculate diagnostic accuracy.
Results: The mean age of the population examined was 54.5±10.5 years; 73% of the patients were male (38 of 52). Overall agreement between the two procedures ranged from 71–96%. The sensitivity, specificity, and positive and negative predictive values of MRCP for anastomotic strictures were 77%, 59%, 79%, and 56%, respectively. The sensitivity, specificity, and positive and negative predictive values of MRCP for common bile duct dilation of >0.7 mm were 64%, 95%, 82%, and 88%, respectively.
Conclusion: Despite significant improvement in the technology to better visualise the biliary system on MRCP, this study found that MRCP does not appear to be sensitive or specific in this chosen population. ERCP should be considered to confirm all positive MRCP findings, and in normal MRCP cases if there are other clinical data suggesting biliary abnormalities.
INTRODUCTION
Magnetic resonance cholangiopancreatography (MRCP) is quickly becoming the gold standard of care in the evaluation of patients who present with laboratory findings that are consistent with cholestasis. Several studies have found MRCP to be both sensitive (>90%) and specific (>90%) for the diagnosis of stones, tumours, and duct injuries.1-5 It has even been suggested that MRCP could replace more invasive procedures, such as endoscopic retrograde cholangiopancreatography (ERCP), for diagnostic purposes in the general population.4
As the number of individuals receiving liver transplants increases, it is important to understand that these previous studies may not apply to patients presenting with cholestasis. There are currently >13,000 patients on the liver transplant waiting list in the USA as of 4th April 2018 according to the United Network for Organ Sharing (UNOS).6 Despite advances in surgical techniques, organ selection, and immunosuppression therapy, the biliary tract continues to be the most common site for postoperative complications.7 Complications such as stricture at the site of anastomosis, stones, and leaks can require long-term therapy and have a significant impact on graft survival and quality of life for orthotopic liver transplant (OLT) patients.7
Patients with biliary complications typically present with cholestatic laboratory abnormalities (elevations in total bilirubin, alkaline phosphatase, and gamma-glutamyltransferase [GGT], with or without elevation in aspartate aminotransferase [AST] and alanine aminotransferase [ALT]). A high index of clinical suspicion must be maintained as these patients are often asymptomatic, without fever or pain due to immunosuppression and hepatic denervation after transplant.8 MRCP is usually completed in these situations to determine the need for more invasive procedures such as ERCP, which can be used diagnostically and therapeutically. The goal of this study was to determine the diagnostic accuracy of MRCP findings in the post-OLT population using ERCP as the gold standard.
MATERIALS AND METHODS
Approval for this study was obtained from the Institutional Review Boards of the University of South Florida and Tampa General Hospital. A retrospective analysis of all patients that underwent an OLT at the University of South Florida and Tampa General Hospital, between January 2012 and April 2015, was performed.
All patients >18 years old who underwent a MRCP and a subsequent ERCP were included in this study. Demographic data were collected, including the age, sex, and BMI of the patients. Presence of anastomotic stricture, common bile duct (CBD) dilation >0.7 mm, bile leak, stone, intrahepatic stricture, or extrahepatic stricture on either modality were recorded as primary outcomes.
In a separate analysis, all post-OLT patients >18 years old who were found to have an anastomotic stricture on ERCP were studied to determine the predictive value of initial laboratory tests for anastomotic stricture. In addition to demographic data (age, sex, and BMI), the presence and severity of any abnormality in temperature, AST, ALT, total bilirubin, alkaline phosphatase, and GGT were recorded.
Endoscopic Retrograde Cholangiopancreatography and Magnetic Resonance Cholangiopancreatography
MRCP was performed using a General Electric 3 Tesla magnetic resonance imaging (MRI) scanner to generate multiplane and multisequence images obtained pre and post-intravenous Multihance® contrast (Bracco SpA, Milan, Italy). ERCP was performed with an Olympus V-Scope™ TJF-160VF side-viewing duodenoscope (Olympus, Tokyo, Japan). Omnipaque™ contrast (GE Healthcare, Little Chalfont, UK) was used for fluoroscopic views of the biliary and pancreatic systems.
Statistical Analysis
Patient characteristics and findings from diagnostic tests were summarised using descriptive statistics and reported as mean and standard deviations for continuous variables, frequency, and percentages for categorical variables. Mann–Whitney U and chi-squared tests were used to compare continuous and categorical variables. The association between categorical variables was summarised as odds ratio (OR), 95% confidence intervals (CI), and mean difference. The Bonferroni correction was applied to adjust for multiple comparisons. The statistical significance for all comparisons was set at 5%. Diagnostic accuracy, measures of sensitivity, specificity, and positive and negative predictive values, along with 95% CI, were also assessed for the compared tests. The agreement between findings on diagnostic tests was also assessed using the Kappa statistic: agreement was considered slight if the κ value was 0.00–0.20, fair if κ was 0.21–40.00, moderate if κ was 0.41–0.60, substantial if κ was 0.61–0.80, and almost perfect if κ was 0.81–1.00. All statistical analyses were performed using SPSS statistical analysis software (Version 22 for Windows, SPSS Inc., Chicago, Illinois, USA).
RESULTS
A retrospective review of 273 patients who underwent OLT at the University of South Florida and Tampa General Hospital between January 2012 and April 2015 was performed. From that group, 52 patients were selected who had previously received an ERCP following MRCP. The mean age of the population was 54.5±10.5 years. The population was predominantly male (73.1%). Average BMI was 27±4.9. The most common primary biliary duct anastomosis type during liver transplant was duct-to-duct (n=50, 96.2%), followed by Roux-en-Y (n=2, 3.8%). The patient population exhibited a number of comorbidities, including hypertension (55.8%), diabetes (32.7%), dyslipidaemia (9.6%), coronary artery disease (5.8%), and chronic obstructive pulmonary disease (3.8%), as well as having a history of alcohol use (44.2%) and tobacco use (65.4%). There were a number of reasons for transplant, including alcoholic cirrhosis (25.0%), hepatitis C virus-induced cirrhosis (40.4%), hepatocellular carcinoma (3.8%), primary biliary cholangitis (3.8%), autoimmune hepatitis (9.6%), nonalcoholic steatohepatitis (7.7%), and other (9.6%).
The most common finding on MRCP was anastomotic stricture in 34 patients followed by CBD dilation in 11 patients. Anastomotic stricture was also the most common finding following ERCP, diagnosed in 35 patients, followed by CBD dilation in 14 patients. Very few patients were found to have bile leaks, stones, or intrahepatic or extrahepatic strictures on either of the two modalities, as summarised in Table 1.
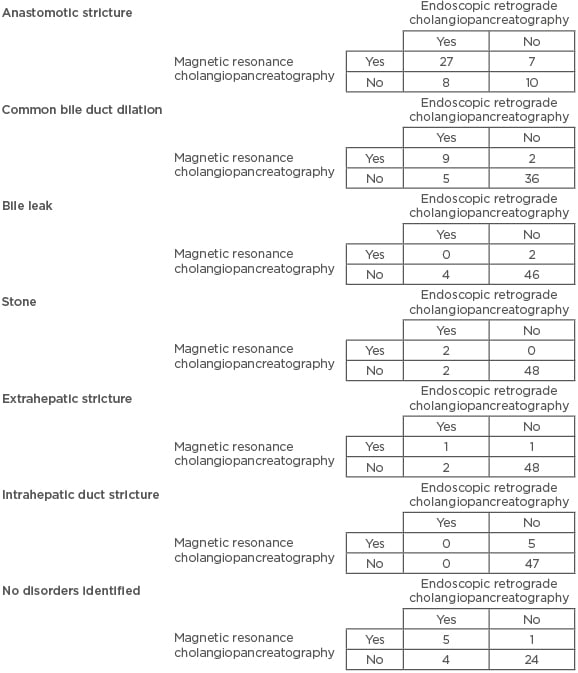
Table 1: Number of patients identified with common disorders following magnetic resonance cholangiopancreatography versus endoscopic retrograde cholangiopancreatography.
The sensitivity and specificity for anastomotic strictures (n=35 on ERCP) for MRCP were 77.1% and 58.8%, respectively, while the positive and negative predictive values were 79.4% and 55.6%, respectively. Agreement between MRCP and ERCP for anastomotic stricture was 71.2%. For CBD dilation (n=14 on ERCP), the sensitivity and specificity of MRCP were 64.3% and 94.7%, respectively, while positive and negative predictive values were 81.8% and 87.8%, respectively. Agreement between the two modalities was 86.5% for CBD dilation (Table 2). With so few cases of bile leaks (n=4 on ERCP), stones (n=4 on ERCP), and intrahepatic or extrahepatic strictures (n=0 and n=3 on ERCP, respectively), we were unable to run diagnostic accuracy calculations between the two modalities.
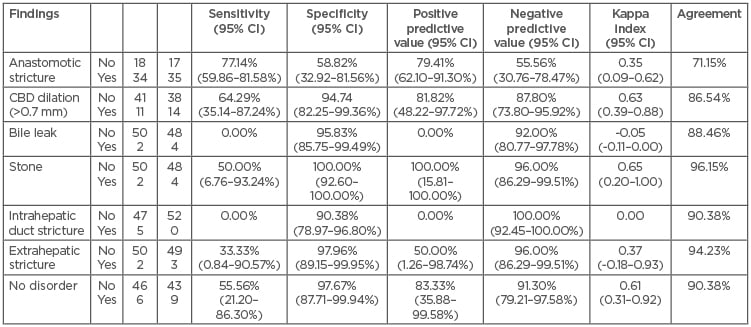
Table 2: Diagnostic accuracy of magnetic resonance cholangiopancreatography.
CBD: common bile duct; CI: confidence interval; ERCP: endoscopic retrograde cholangiopancreatography; MRCP: magnetic resonance cholangiopancreatography.
A subgroup analysis was completed in 56 patients after selecting the individuals who underwent an ERCP that was either normal or had an anastomotic stricture, in an attempt to determine if the presence of, or the severity of, laboratory abnormalities, such as temperature, AST, ALT, total bilirubin, alkaline phosphatase, and GGT, could help predict anastomotic strictures. A total of 19 patients had normal findings on ERCP (normal group) and 37 patients had an anastomotic stricture (stricture group). Mean alkaline phosphatase levels were higher in the stricture group versus the normal group (mean difference: 253.6 U/L; 95% CI: 2.45–504.81; p=0.048). Severe elevation of alkaline phosphatase (>301 U/L) had an OR of 4.53 (95% CI: 1.13–18.24; p=0.05) for anastomotic stricture. Severe elevation in total bilirubin concentration (>4.1 mg/dL) and any abnormal GGT value had a greater OR for anastomotic stricture; however, this was not statistically significant, with an OR of 2.05 (95% CI: 0.64–6.56; p=0.35) and 4.25 (95% CI: 0.36–50.39; p=0.55), respectively (Tables 3 and 4). Complications within 14 days of ERCP included pancreatitis (n=1), stent migration up (n=1), and stent migration out (n=1).
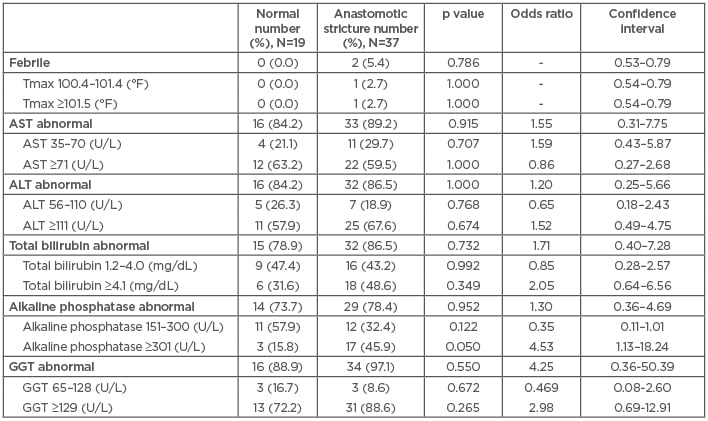
Table 3: Laboratory findings in patients with normal and abnormal endoscopic retrograde cholangiopancreatography.
ALT: alanine aminotransferase; AST: aspartate aminotransferase; GGT: gamma-glutamyltransferase; Tmax: maximum temperature.
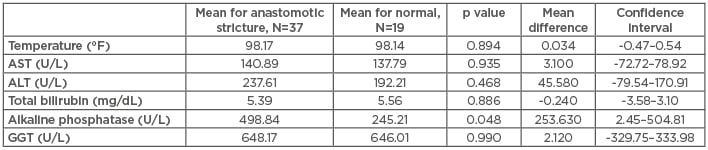
Table 4: Average values of laboratory findings in patients with normal and abnormal endoscopic retrograde cholangiopancreatography.
ALT: alanine aminotransferase; AST: aspartate aminotransferase; GGT: gamma-glutamyltransferase.
DISCUSSION
MRCP has substantially improved the ability to view the biliary system with radiographic imaging. New technology even allows for three-dimensional (3D) imaging that can be reformatted to produce a rotating display to analyse the biliary tract from any angle.9 This study found that MRCP was not sensitive or specific at evaluating the biliary system in the post-transplant population. Furthermore, it was discovered that a negative MRCP was essentially no better than chance at diagnosing an anastomotic stricture, with a negative predictive value of 56%. There were eight cases when an anastomotic stricture, defined as focal narrowing at the site of anastomosis with contrast injection as observed by the endoscopist, would have been missed if ERCP had not been performed in the setting of a negative MRCP. Aydelotte et al.10 found similar results evaluating the use of MRCP for discovery of choledocholithiasis, duct strictures, and duct injuries. The group advocated for the removal of MRCP as a diagnostic tool for the work up of biliary duct pathology.10 It is also important to note that two patients had Roux-en-Y hepaticojejunostomy biliary reconstructions. Both of these patients had anastomotic strictures on ERCP. The remaining patients included in this study all had duct-to-duct biliary reconstructions.
Several studies claim that MRCP is equally as accurate as ERCP; however, these studies focus on the evaluation of biliary duct pathology in the general population.5,11,12 Katz et al.13 studied 27 post liver transplant patients and found a much better sensitivity and specificity between MRCP and ERCP (93% and 97.6%, respectively). However, only 18 of these patients underwent both procedures. They found one false negative and one false positive in the 18 selected patients.13 Aufort et al.14 studied 27 patients who underwent MRCP and ERCP after liver transplantation and found a sensitivity and specificity of 85% and 81%, respectively. However, their study included a much more detailed review of MRCP images at a later date by dividing the biliary tree into seven segments, and the study also had two blinded independent reviewers. Radiologists do not have the ability to perform such a detailed reading of MRCP images in clinical practice.14
Missing a stone or a delay in diagnosing a malignancy will typically result in continued pain and worsening cholestatic laboratory findings, eventually leading to diagnosis via ERCP at a later time in the general population. In the liver transplant population, delay in discovering biliary pathology, especially anastomotic strictures, can lead to severe infections, organ failure, and potentially death.
In this study population, MRCP was found to be not as useful as anastomotic evaluation, and the procedure is difficult in most patients due to duct mismatch post-transplant, which makes it difficult to determine whether anastomotic narrowing is significant. During ERCP, the endoscopist has the option of timing drainage or sizing the anastomosis with occlusion balloons to more accurately determine presence and severity of stricture and, ultimately, determine need for intervention. Additionally, the subgroup analysis carried out here was intended to determine if the severity of certain laboratory abnormalities would help clinicians predict the possibility of anastomotic stricture; however, none proved to be a reliable enough predictor.
Limitations
A limitation of this study is that it was performed as an observational retrospective study. The goal of this study was to determine diagnostic accuracy, but despite the 273 OLT patients evaluated at our centre, 83 of which had an MRCP, only 52 fit the study criteria of undergoing MRCP followed by ERCP and so were selected for in-depth study. This generated a selection bias, as a small number of patients with normal MRCP scans (n=6) did undergo a subsequent ERCP due to significant clinical suspicion for biliary abnormality. While a prospective study would reduce the level of bias, it was not feasible, and to subject all patients with any suspicion of biliary disease to both procedures would be unnecessary, costly, and potentially dangerous. Additionally, a single clinician performed the chart review and outcomes were measured based on procedure notes, which can result in reader error.
CONCLUSION
In conclusion, MRCP does not appear to be either sensitive or specific in discovering biliary tract pathology in the post liver transplant population. ERCP should be used to confirm all positive MRCP findings, and even in normal MRCP cases if there are other clinical signs to suggest biliary abnormalities.






