BACKGROUND
Primary biliary cholangitis (PBC) management in Europe has undergone a significant transition following the European Medicines Agency’s (EMA) withdrawal of obeticholic acid1 and the subsequent approval of peroxisome proliferator-activated receptor (PPAR) agonists.2,3
AIMS
To address this overhaul in second-line therapies, the authors launched an educational initiative to increase gastroenterologists’ and hepatologists’ competence and confidence in using second-line therapy and assess their subsequent actions in clinical practice.4
METHODS
Physicians participated in a 38-minute, debate-style online continuing medical education (CME) activity on (re-)evaluation for second-line PBC therapy. The educational effects were measured in two phases: part A involved activity pre- and post-assessments, while part B was a Moore’s Level 5 performance survey completed 30 to 60 days after participation.
RESULTS
Of 1,413 gastroenterologists/hepatologists who had engaged with the programme, 58 completed all questions in part A and 33 in part B. Of which, 52% were community practitioners, 39% in academic settings, and 8% other.
Part A revealed significant improvements in physicians correctly identifying patient age and liver stiffness as critical indicators for second-line treatment, factors that were previously underestimated (pre-assessment: 16% correct versus post-assessment 45% correct; p<0.001). Furthermore, physicians demonstrated an increased understanding that PPAR agonists improve patient itch and biochemical responses, normalising alkaline phosphatase (pre-assessment: 62% correct versus post-assessment 76% correct; p<0.05).
This knowledge translated directly to increased confidence. While 84% of participants recognised they had patients requiring reassessment, 36% demonstrated measurably improved confidence in determining exactly which patients should be evaluated following the activity.
The programme subsequently successfully drove meaningful changes in clinical practice. The follow-up survey in part B revealed that 94% of respondents modified, implemented, or reinforced a clinical practice as a direct result of the education. Figure 1 outlines the specific practice changes implemented by specialists 30 to 60 days after the educational intervention.
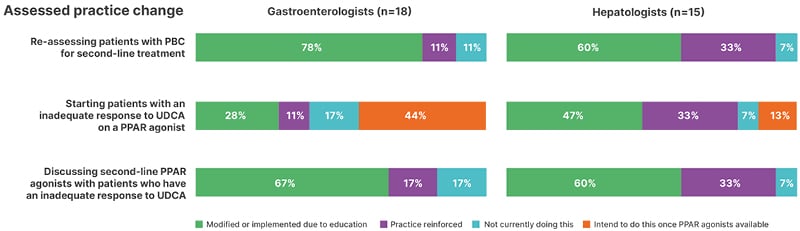
Figure 1: Physician practice changes post-education.
PBC: primary biliary cholangitis; PPAR: peroxisome proliferator-activated receptor; UDCA: ursodeoxycholic acid.
Despite the high rate of overall reassessment (91% actively reassessing patients), physicians reported practical barriers that limit broader implementation. The primary barriers cited were capacity challenges related to scheduling patient clinics and difficulties in securing access to PPAR agonists.
CONCLUSION
Ultimately, the CME activity successfully boosted practitioner confidence and catalysed active reassessments of patients with PBC. Moving forward, continued education must focus on closing the gap between simply monitoring patients with PBC and actively prescribing these new second-line treatments by reinforcing clinical indicators and the expected benefits of PPAR agonists.





